


Protons for Prostate Cancer: 2772 patients! Outstanding results in a retrospective setting.
So do the results hold up? Strong data leads to more questions than answers

For this one, what I thought we would do is look at every criticism of the concept of treating prostate cancer with protons on Twitter and just go one by one. A matched cohort analysis of 2772 patients to 2772 tweets. Joke! Couldn’t help myself.
Instead, what I thought we’d do was look at this study and compare it to IMRT, FLAME SIB and SBRT data - as best we can and look for insight. It is retrospective single institution data but I think the size of cohort makes it quite important to attempt to file in with other historical data points.
Is it randomized? No. Can we make real / clear recommendations from this publication? No. Can you answer the all-important question regarding photons vs. protons? No. But I do think we can look around at big data points and file this thing pretty well. Prostate cancer just works like that.
So yes, randomized trials are needed - I wrote that. And I’m on record that as designed, I think it is highly unlikely that the COMPPARE trial will be positive and even if positive, it will be dismissed via pretty reasonable and rationale perspectives. Does this make me think I might be too pessimistic? Maybe, a little, but I’m staying put on my predictions. So with that context, let’s go.
Today we’ll be more data driven, more references, just to emphasize that aspect of the work here.
In total over 40 studies considered to give this current data context.
I’m hoping a broader look across our landscape is helpful. I think it will be educational for me as I’ll spend a few weeks considering the various datasets and thinking about how best to compare this result to prior publications. Maybe an exercise in futility, maybe not. As always, up to the reader to decide.
The focus today will be largely on intermediate risk disease. I’m going to reserve a focused look on high risk for a different article as everything changes when we look at Pelvis / No-Pelvis and add ADT routinely per the POP-RT trial. (Issues which were previously discussed here).
And so we begin:
IMRT:
An early article on this Substack summarized our historical IMRT literature. It is worthwhile to at least click over and cross reference as you read this one.

It covers 26 important historical references as I attempted to summarize IMRT dose schedules and various trials that led to our current “standard of care” options. It is, in a way, my personal walk through the history of dose escalation and then through to moderate hypofractionation.
Here is one of the summary statements:
My argument is simply this. We have room to improve. Anything shorter that was compared to traditional fractionation cannot be expected to have outcomes any better than 80%-85% (the above data covers 11 trials - mostly prospective data). And depending upon your patient population, you’ll likely need significant ADT to get that result. If you want to do these types of approaches and want to get closer 90%, you need to treatment almost every intermediate risk patient with ADT.
So just pencil in something in 80s for IMRT with standard of care dosing with adequate Phoenix follow-up (defined per the original reference paper (1) as 24 months longer than reported metric - ie 7 yrs of follow-up to report 5 yr data).
Again, good data - lots of references to get to this point - too many to include again here today.
FLAME - SIB 35 fraction integrated boost approach:
I want to discuss this as it is a randomized prospective dataset. It is multi-institutional, IMRT based and therefore - clearly - the strongest type of data - better than a retrospective look (2). The problem here is, honestly, the patient cohort is too high of risk patients. And they integrate ADT (very appropriately but still makes direct comparisons difficult). The great part of the trial to me is that they used ADT more sparingly - the trial was 84% high risk with ONLY 65% of the patients receiving ADT - so more than 20% with high risk were not treated with ADT.
Why include this trial - High risk with ADT usage?
Because I strongly believe that if I just used IMRT US standard of care dosing and said, 80%-85% outcomes - people would think I was biased. And to some degree that would be correct because I do think this trial clearly shows that you can do better with IMRT - if you don’t proceed along standard uniform dosing approaches.
SIB in this trial demonstrated clear improvement with dose escalation that was safe. Therefore, to me, this approach supplants traditional IMRT as the bar that needs to be cleared - be that with photons, protons, SBRT, or brachytherapy.
At 5 yrs, the bDFS was 92% in the SIB arm and 85% in the “standard” arm - a 7% difference. The rate of failure was basically cut in half with more dose. Compare that to much older Cleveland Clinic data (3,4) that established one of the primary approaches we use today - 75% for HR in the 70 Gy / 28 fx Cleveland Clinic data vs. 92% in the SIB arm here. Sure there are timing issues related to stage migration, imaging differences, and improvements with IMRT and our knowledge base; but the failure rate for the 70 Gy / 28 fraction approach is over 3x higher. And ADT is about the same or even less in FLAME. So I think it is a bit unfair to look only at NCCN “standard of care” dosing, and to me, and describe global IMRT results.
That said:
Do most use NCCN “standard doses” for intermediate risk? Yes.
Do I think we have proven those standard doses can be surpassed? Yes
So, here with higher doses delivered to the disease the high watermark is raised. Potentially up to or around 90% or even a bit above 90%. But we have to make two difficult translations: 1) lower the risk cohort to IR disease, and 2) drop ADT.
Just to close the book on IMRT, I’ll go back to PACE-B (5). Pretty darn bright people running darn well executed trials. Great scientists working as a team to accomplish great trials - not some blogger with one opinion on Substack :) Read the power calc below:

Just to re-iterate: IMRT according to these experts is anticipated to achieve 85% control if you don’t include ADT in a lower risk segment of intermediate and low risk patients. As a reminder, here are the entry criteria for PACE B: (Low risk and a rather favorable cohort of intermediate risk disease - should be pretty small set of UIR disease)
Low Risk: (meet all)
Clinical stage T1c – T2a, PSA <10 ng/ml, Gleason score ≤6
Intermediate Risk: (have one)
Clinical stage T2b-T2c, PSA 10 – 20 ng/ml, Gleason score 3+4
And even here, remember that same panel of experts raised the dose for the “standard” arm above “standard” doses to 62Gy/20 fractions. They raised the dose due to a lack of ADT despite a very favorable cohort knowing that, without the dose-escalation, they might struggle to meet 85% control.
So, from my perspective, my “counter-narrative” position that NCCN dosing is too low for many with IR disease is actually quite well established.
Summary: FLAME SIB likely gets us to 90% or so. As reviewed, it is very difficult to lower the cohort risk profile and adjust for ADT - so yes, it is a guestimate. But I think it demonstrates that higher doses achieve higher control rates even against current dose recommendations. If you don’t like guestimates, use 82%-85% for IMRT.
SBRT:
Here we’ll focus on two large datasets - each are large series representing a number of institutions and a number of publications but I think if you start there, add in one current trial, and look ahead to PACE B data, you are up to speed pretty quickly.
First Large SBRT Dataset:
The paper presents a headline figure of 95% control, but if you disregard low risk disease and dig beneath the surface, it is quite a different picture - at least on my review. So I need to spend a bit of time and explain why you can’t just write down 95% for SBRT.
Here is summary of the individual trial data for intermediate risk disease:
Widmark - largest number of IR patients. Seven fractions - not the magical 5 but ninety percent of the trial was IR achieving 83.7% control. Prospective, randomized, but follow-up is only 5 yrs - so the outcomes will further deteriorate.
Meier - 137 IR patients at 95% bRFS. Gave 40/5 and unfortunately, follow up is only 61 months - so a full 2 yrs short of recommended to report 5 yr results.
Katz - 153 IR patients at 90% bDFS. Follow-up 6 years.
Fuller* - 147 IR patients - at 5.5 yrs median follow-up FIR 92% and UIR 83%.
The remainder of the datasets are very small: Mantz 33 men only very FIR. Alayed 12 men with IR (see next big dataset for better group from same author) and Boike 27 IR men treated on dose escalation trial that cause too much toxicity per authors. Exclude Boike and you have an additional 45 very favorable men to consider.
And that is a quick summary of the intermediate risk disease in that meta-analysis.
Like I said, the headline number is 95% but read the trials, do your own math, and I believe you will come away with the impression that for IR disease. Widmark is low / mid 80s. Fuller UIR is 83% reported with 18 months too short follow-up. You have one early reported dataset at 95% - strong results but limited duration follow-up and 40/5 so more dose.
Second Large SBRT Dataset:
This is 2142 men from 10 single institution trials from just earlier in 2019 - published 2 months prior to the above analysis. Median follow-up was 6.9 years. Minimal ADT use with around 7%-8% of intermediate risk men receiving ADT (impressive and quite bold from my perspective). Per abstract, FIR is bDFS is 91.4% 7yr and 85.1% for UIR. Failure rates were Phoenix definition. All prospective patients. 5 year rates (7 yr median follow-up) appear to be just above 90% (~92%) for FIR and just below 90% for UIR (~88%). 5 year taken estimated from the KM curves:
FIR ~92% (ADT 6.8%)
UIR ~88% (ADT 9.4%)
It is a great study - amazing reference dataset. It supports an bRFS around 90% for intermediate risk disease with rational and appropriate conclusions. Very low nadirs - excellent kinetics.
To me, this is one to use - take the abstract numbers and write it down. Simple.
(Most of this data is then supported further in the more recent Refining the definition of biochemical failure in the era of stereotactic body radiation therapy for prostate cancer: The Phoenix definition and beyond. (16) < this paper is a great source of PSA kinetics for SBRT - a consistent reference paper to me - largely the same patient population.)
So if you drop out low risk disease, these two large papers include about 1300 men demonstrating SBRT obtaining biochemical relapse free control rates for intermediate risk disease of approximately 90%.
And it is supported by this trial that came out in 2023.
This is a multi-institutional trial of 170 men. Briefly, 22% were low risk, 63% were IR, and 15% were high risk. About 45% of the cohort received ADT.
At median follow-up of 78 months, biochemical failure was observed in 14 patients in the EOD arm and in 7 patients in the QW arm with a 5-year biochemical relapse-free survival rate of 92.2% and 93% for arms A and B, respectively (P = .13). And notably, it didn’t push dose. This was a urethal sparing 3625 cGy / 5 fraction trial.
Why is this one higher - actually above 90% with good follow-up duration? Likely because ~45% receive ADT moving a “real” unadjusted answer of 89%-90%. (~3% improvement based on ADT volume my estimate) - the reality of ADT. I discuss the trial in quite a bit of depth in this full article on this paper. I point out some quibbles and I still personally lean on the Consortium Data as the more robust, “best example” of excellence within SBRT results to date - but this is a strong dataset that I see as slightly surprising on the upside due to dose level in IR disease.
For a week or two, I considered whether this trial result should move my predictions for PACE-B from 88% to 90%, but I ended up staying put based on quibbles and nuance. But if PACE-B returns at 90%-92%, this trial would support that data. If PACE-B returns at 99% for the SBRT arm… well, I owe someone a dinner (inside joke, but to date, still feeling quite confident it won’t hit that mark - reference for joke below).

So SBRT for non-low risk disease is perhaps as high as 90% - higher if you add in dose or ADT. I think PACE-B will be the measuring stick and, like I have said, they are pretty bright and set the goal as 85% for a more favorable intermediate and low risk cohort. I’m on record predicting 88% for PACE-B. Time will tell.
In summary, we’ve covered some ~1400 IR patients treated with SBRT pretty quickly. Read the links / references if you want to go much deeper.
Me? I write on back of napkin,
Intermediate Risk:
IMRT ~85%
SBRT ~88%-92%
SIB or higher dose SBRT approaches 90%-93%.
(Assuming less selected IR groups with minimal to no ADT)
Protons:
So now we are to the current trial out of MD Anderson.
Proton Therapy for the Management of Localized Prostate Cancer: Long-Term Clinical Outcomes at a Comprehensive Cancer Center (18)
As we all know, this study’s downfall is that it can suffer from unknown bias in the patient cohort - a more affluent group that will do better beyond our “standard” risk assessments. But it has very large patient numbers with 2772 men treated.
And really none receive pelvic treatment - like none - 28 total with 15 in the very high risk cohort. Median follow up is 7 years so I’ll focus on the 5 year data.
YAY - excellence in follow-up duration!!
ADT usage in this study is significant. And relative to outcomes in the SBRT Consortium cohort, it is much broader ADT usage. I include the associated percentages below from the paper. And kinetics. Really it presents no kinetics with the only data point presented being a median PSA at 7 years of 0.3.
Outcomes for prostate cancer treated with Protons at MD Anderson:
LR: 98.2% (11% ADT)
FIR 94.2% (42.5% ADT)
UIR 94.3% (82.1% ADT)
HR 86.1% (100% ADT)
VHR 68.5% (100% ADT)
*glances back at napkin and thinks, “well that is interesting.”*
FIR and UIR is where I’ll focus. 94%. Simply one of the strongest numbers in print for that risk cohort.
(Yes I remember 95% (90% DFS) in POP-RT but we’ll come back to HR later).
Follow-up is strong - median 7 years to report 5 yr data - with very large numbers of both FIR (850) and UIR (851)patients. In fact, this single report includes more unfavorable risk than the above large scale collection of SBRT data. I do think, compared to the Consortium data where very little ADT was utilized, we should drop 2%-4% for more equivalent comparisons. And if you do that, it nearly mirrors a 92%, 88% outcome in that publication. (all ADT to none is approximately 5% difference historically at 5 years)
So clearly this is a large series with excellent long-term outcomes - really some of the highest in print (with the caveat of more ADT usage but truly excellent median follow-up duration).
Compared to hypofractionated IMRT “standard of care” uniform dosing recommended via NCCN, these are simply superior results to anything in our literature I can find.
And this is now NOT a one off publication. It is supported by the University of Florida data: 8 year median follow-up (19). Again note the long / appropriate follow-up duration.
UFPT Data: (5 and 7 yr data respectively):
LR (98.8% / 98.8%)
FIR (97.2% / 95.2%) – (3.3% ADT) 5 of 149 received ADT
UIR (93.1% / 88.8%) – (7.3% ADT) 12 of 164 received ADT
And the Takagi publication (21) (84 months median follow-up):
LR 99% (11% ADT)
FIR 93% (22% ADT)
UIR 90% (52% ADT)
Wow. Pretty consistent. Again, in contrast to the non-proton data, this appears to be 90% or above at 5-7 years out for IR disease with 7-8 years median follow-up. A metric that has been difficult to achieve with this reported level of consistency outside of protons.
Granted, these three centers still represent a minority of prostate cancer patients treated with protons, but the data within these publications are quite consistent. So today, in three rather large publications with great follow-up duration, we have really strong data.
Just for kicks - my 262 patient database now (late August) has a median 1 yr PSA of 0.34 (mean 0.84) and a 2 yr median PSA of 0.27 (mean 0.42). And I’ve documented over and over that I’m attempting to be more similar to the UFPT data in limiting ADT usage for intermediate risk disease (my use is falling as I gather more data - currently giving ADT in about 1 in 4 with UIR). Follow-up in my personal database is short (19 months), but PSA kinetics are PSA kinetics and these are trending towards strong results not inconsistent with these two published series. I get a bit nervous putting this info out there because the numbers in print are so very high for control and one can’t be sure mine will be quite mirror these studies with longer follow-up, but the kinetics are strong and I’m pleased to date that I’m at least close.
My personal OKC Intermediate Risk PSA kinetics:
IR: 0.6 at 1 yr: 0.4 at 2 yrs (144 men: 22 ADT)
FIR at 0.8 at 1yr: 0.47 at 2yrs (72 men: 2 ADT)
UIR at 0.39 at 1yr: 0.3 at 2 yrs (72 men: 20 ADT)
In general I’ve argued <1 at 1 yr and <0.5 at 2 yrs is on pace for 5 yr DFS>90%. (Note that assumes appropriate Phoenix definition follow-up and is disease free survival, not biochemical disease free survival - at least for pre-PSMA data).
I’d also note that since moving to 7250 cGy(RBE) / 29 fractions from 7920 cGy(RBE) / 44 fractions, my kinetics are stronger - meaning faster to lower - consistent with about 5% more dose.
So the question becomes:
Why are the proton results so strong even compared to single center non-randomized data? It doesn’t make sense?
That really is the question - look at the single institution IMRT data - nothing gets close to this mark. Brachy has (20) but we all realize there is at least some pretty strong selection in that setting - but it clearly can produce excellent results. SBRT vs proton comparisons in non-randomized settings should be pretty similar - both will be biased attracting slightly different cohorts of patients than rural low volume centers, and today, each are compelling and appear to be potentially superior approaches to our historical dosing patterns with photons.
I’m sure there is bias in the basic cohort but realistically, proton centers treat prostate cancer with protons - not some of them - all that walk in. There is no selection once they reach the facility (other than bilateral hip cases). So yes, there is some selection but far less than in many implant series and less but different than SBRT series in most series.
I wrote this in March with regards to the Florida data which at the time stood alone in the US market- trying to answer why it appeared different:
And I’m not certain either and that argument, one that simply says it doesn’t quite match history, to me, is as strong as any. Run studies 100 times and you will see outliers. Such is life.
But today, with three large datasets - two in the US and watching as my own personal database matures, I think that argument weakens and I think one should, at a minimum, begin to consider alternative answers - that protons may in fact allow for “easier” high dose treatment. Here are my primary thoughts for a true positive difference:
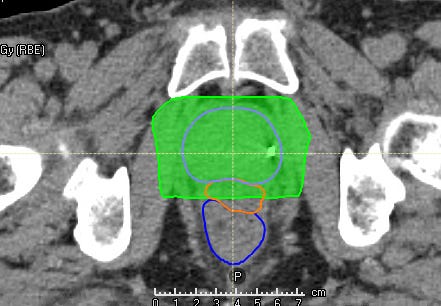
In passive scanning, there is nearly NO tradeoff on dose to prostate / margin coverage around the regions of the neurovascular bundles. With IMRT, this region IS the decision point - narrower lowers rectal dose but is tighter. With passive scanning, you get this big rectangular dose box - it is different (ex shown below). (I actually worry about this in new centers starting with PBS - in fact, if I were running a PBS prostate program, I would mirror a passive scanning dose pattern - purposefully and NOT attempt to mirror an IMRT dose cloud).
In the Florida series (and in my more recent patients), the base dose is approximately 5% higher while also often delivering 6000 cGy (RBE) / 24 to the seminal vesicles - this dose escalation might result in some improvement.
The simple RBE assumption of 1.1 might too low and therefore result in an error of 5% resulting in more delivered dose to target.
There is some photon particle effect that lowers the alpha/beta for prostate cancer when treated with protons compared to photons. I believe this should be quite small - even a relative move in the effective alpha / beta from 2 to 1.2 results in only a ~2% difference in EQD2 using these more protracted schedules.
Conclusions:
Obviously the final answer will be randomized data. Unknown confounders and biases are impossible to otherwise remove. Further, staging requirements, how you follow people, how often you draw labs, ADT usage and when you integrate PSMA scans all can impact results. This is all straightforward.
(That’s why I’ve argued for us to clearly address these types of issues today - to allow for earlier and quicker comparisons of approaches (think HIFU / TULSA). As an example, my last 3 failures are all prior to Phoenix failure based on smaller but patterned moves in PSA paired with PSMA scans - times are shifting quickly and we should be working to stay ahead of the curve to keep the integrity of our data. This underlies the rationale for my focus on kinetics.
And yes, I understand shortening the lab intervals and earlier PSMA scans makes my data “worse” - but my goal is early discussion of salvage options - I think early salvage discussion is likely quite valuable. In fact, as I write this, I’m going to begin to track 3 outcomes - Phoenix fail, any fail, and fail resulting in systemic treatment for this very reason).
But as I’ve argued on this site, from my perspective, we simply need to prioritize dose and cure rates, and from my perspective, while minimizing ADT. If you obtain great kinetics at 1 yr and 2 yrs - that point towards long-term high control rates - say in excess of 90%, it doesn’t really matter to me how you get there. If that means IMRT with an SIB approach with more fractions or an SBRT approach or protons or brachy - I’m good. First get great results and limit the over treatment with ADT recommended in our guidelines.
(I would note, the MDACC results are strong enough, late enough - 7 years of follow-up - crude failure rate for 2772 men of ~5%, that it makes me reconsider ADT use percentage goals for younger men with UIR disease.)
And yes, if all approaches get there equally easily and with equal toxicity risk regardless of patient volumes and “nuance” in the process, then yes, ultimately costs come into play (and that balance point is different in different world markets with different levels of capital and machine access). But to me, our specialty should simplify and focused on excellence in outcomes as our priority.
I don’t have the answers. The results from both Florida and MD Anderson surprise me a little bit - both seem awfully strong relative to our historical data. Likewise, I think you can look at the Consortium data and with adjustments for ADT make an argument that it too lies in a similar ballpark - each potentially “just superior” approaches to what we have done.
My personal experience is consistent with strong PSA kinetic results to this point and four and one half years into working at a proton center, I trust a 7250 cGy (RBE) / 29 fraction approach over a proton SBRT approach or my prior uniform IMRT approach with respect to PSA response, PSA nadir and toxicity. Simply it works and I really do believe I see lower numbers today.
As I’ve argued before, we have various options to achieve great results, but we need to push to achieve them and this is why I argue for a reassessment of NCCN dosing schedules - they aim for 85% when I believe we can do better very safely today.
Kudos to the authors for publishing the data in a controversial use area of our specialty. This data adds to our knowledge base and I think we are clearly better off to have it available. Kudos to the experts across our field who demonstrate great results in the treatment of prostate cancer! I love the work by those that limit ADT usage and still demonstrate excellence in long-term outcomes - many of which, we covered today (As a reminder, the Consortium SBRT report and UFPT each gave <10% ADT in UIR disease and each reported outstanding outcomes!) At the same time, in ways, 94% control for UIR makes perhaps the strongest argument in favor of 6 months of ADT that I have seen in our literature.
The COMPPARE trial (22) closed October 31st, 2022 with accrual of 2524 men and some data might be available as early as next year. Between that randomized prospective dataset and PACE-B, we’ll be a lot more informed as to where we stand today next year. Whether this study is deemed, in the long-term, to be supportive of those randomized trials or an example of the power of retrospective publication biases is yet to be determined.
Looking forward to an exciting year of progress as we keeping searching for better. Thanks as always for following along. Next week, a paper looking at biochemical failure landed - it brought back memories and ties in nicely with the conclusions above. Until then.
*Note on Fuller data: Two publications - the earlier publication is actually within the meta-analysis but even in the longer follow-up “10 year” paper, they report a median follow-up of 5.5 years. Again per Phoenix, median follow-up should be at least 7 yrs for 5 yr results. So I present the 5.5 yr median follow-up results above - and even in that publication, follow-up is insufficient and results should deteriorate with longer follow-up.
REFERENCES:
Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference
https://www.redjournal.org/article/S0360-3016(06)00663-8/fulltextFocal Boost to the Intraprostatic Tumor in External Beam Radiotherapy for Patients With Localized Prostate Cancer: Results From the FLAME Randomized Phase III Trial
https://pubmed.ncbi.nlm.nih.gov/33471548/Hypofractionated Intensity-Modulated Radiotherapy (70 Gy at 2.5 Gy Per Fraction) for Localized Prostate Cancer: Cleveland Clinic Experience - 5 yr
https://www.redjournal.org/article/S0360-3016(07)00535-4/fulltextTen-Year Outcomes of Moderately Hypofractionated (70 Gy in 28 fractions) Intensity Modulated Radiation Therapy for Localized Prostate Cancer
https://www.redjournal.org/article/S0360-3016(19)30182-8/fulltextPACE Trials (Intro should be required reading for residents pg: 10-21)
https://www.icr.ac.uk/media/docs/default-source/default-document-library/pace_protocol_v12_clean.pdf?sfvrsn=130f3069_0Stereotactic Body Radiation Therapy for Localized Prostate Cancer: A Systematic Review and Meta-Analysis of Over 6,000 Patients Treated On Prospective Studies
https://pubmed.ncbi.nlm.nih.gov/30959121/Stereotactic body radiotherapy as treatment for organ confined low- and intermediate-risk prostate carcinoma, a 7-year study - Katz
DOI: 10.3389/fonc.2014.00240Multicenter Trial of Stereotactic Body Radiation Therapy for Low- and Intermediate-Risk Prostate Cancer: Survival and Toxicity Endpoints - Meier - Cyberknife data
https://pubmed.ncbi.nlm.nih.gov/30191864/Virtual HDR CyberKnife SBRT for Localized Prostatic Carcinoma: 5-Year Disease-Free Survival and Toxicity Observations - Fuller
DOI: 10.3389/fonc.2014.00321High Dose “HDR-Like” Prostate SBRT: PSA 10-Year Results From a Mature, Multi-Institutional Clinical Trial - Fuller Mature
https://www.frontiersin.org/articles/10.3389/fonc.2022.935310/fullA Phase II Trial of Stereotactic Ablative Body Radiotherapy for Low-Risk Prostate Cancer Using a Non-Robotic Linear Accelerator and Real-Time Target Tracking: Report of Toxicity, Quality of Life, and Disease Control Outcomes with 5-Year Minimum Follow-Up - Mantz
DOI: 10.3389/fonc.2014.00279Dose escalation for prostate stereotactic ablative radiotherapy (SABR): Late outcomes from two prospective clinical trials - Alayed
DOI:https://doi.org/10.1016/j.radonc.2018.03.005Phase I dose-escalation study of stereotactic body radiation therapy for low- and intermediate-risk prostate cancer - Boike
https://pubmed.ncbi.nlm.nih.gov/21464418/Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial - Widmark
DOI: 10.1016/S0140-6736(19)31131-6Long-term Outcomes of Stereotactic Body Radiotherapy for Low-Risk and Intermediate-Risk Prostate Cancer
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6484596/Refining the definition of biochemical failure in the era of stereotactic body radiation therapy for prostate cancer: The Phoenix definition and beyond - Ma Consortium based
https://pubmed.ncbi.nlm.nih.gov/34774650/Every-Other-Day Versus Once-a-Week Urethra-Sparing Prostate Stereotactic Body Radiation Therapy: 5-Year Results of a Randomized Phase 2 Trial
https://www.redjournal.org/article/S0360-3016(23)00301-2/fulltextProton Therapy for the Management of Localized Prostate Cancer: Long-Term Clinical Outcomes at a Comprehensive Cancer Center
https://www.thegreenjournal.com/article/S0167-8140(23)89748-1/fulltextFive- and seven-year outcomes for image-guided moderately accelerated hypofractionated proton therapy for prostate cancer
https://pubmed.ncbi.nlm.nih.gov/34965846/Proton Therapy for Localized Prostate Cancer: Long-Term Results From a Single-Center Experience
https://pubmed.ncbi.nlm.nih.gov/33186616/High dose brachytherapy as monotherapy for intermediate risk prostate cancer
https://pubmed.ncbi.nlm.nih.gov/22088340/COMPPARE TRIAL:
https://radonc.med.ufl.edu/researchlabs/current-radiation-oncology-research-at-uf/research-programs-2/