
Prostate SBRT: 92%+ Control. Prospective Multi-institutional data
New trial - new data. A look back at my predictions and a look forward.

www.protons101.com
Home to the musings of a radiation oncologist - with a slant on protons and dose and optimizing cancer outcomes.
Medicine moves so very quickly today. Every day, somewhere there is new data released and occasionally it is pretty valuable. Today we’ll look at a new dataset just published that demonstrates excellent control with SBRT treatment for prostate cancer using a relatively low dose approach.
Part of the goal of this Substack is to attempt to bring a balanced look at our field and our approaches. Part of that requires me to look back and see how I did - call balls and strikes - hopefully accurately and if and where I was right or wrong, highlight some of those points.
Urethral Sparing Prostate SBRT:
And there is a new trial out that I think is good enough to require a deeper look:
Every-Other-Day Versus Once-a-Week Urethra-Sparing Prostate Stereotactic Body Radiation Therapy: 5-Year Results of a Randomized Phase 2 Trial (Ref 1)
The trial is published online as of March 29th, 2023 so a little over a month old but I believe it sets a new high water mark for a prospective multi-institutional SBRT publication in non-low risk disease achieving a disease free survival in excess of 92% at 5 yrs. At least those are the headlines, today we’ll look a bit closer and review what we’ve discussed previously here on this Substack.
The trial presents 5 year results from a prospective, multicenter phase II trial comparing every other day SBRT radiation to once a week SBRT radiation in 170 men. Both arms utilize 3625 cGy in 5 fractions and both limit the urethra to 3250 cGy. Median follow-up was 78 months. Margins are 5mm except posteriorly at 3mm and a endorectal balloon was used for most patients. Urethra was urinary catheter +3mm margin which was then kept below 3250 cGy.
In summary acute toxicity was limited. GU toxicity was Gr1 or zero in 76% of men with GI toxicity was Gr1 or zero for ~90% of men. There was no difference in toxicity between the two approaches. Biochemical failure at 5 years was 92-93% between the two arms.
An Upside Surprise?!
My initial take is this is better than I would have estimated based on all the work I’ve done buried in our prostate literature for two months now. Yay!!
The trial it is a relatively diverse patient population across our risk spectrum as shown in this portion of Table 1.
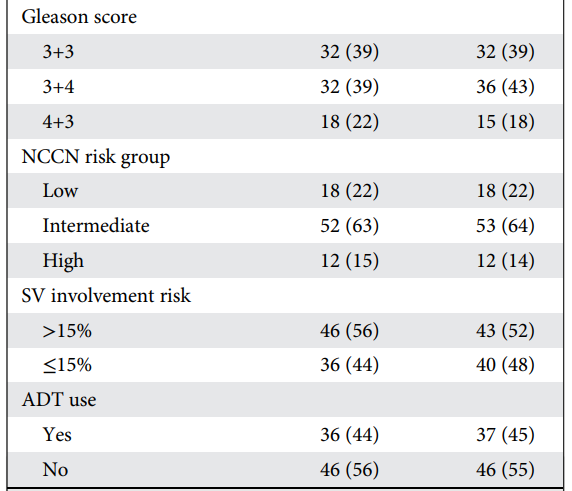
Per the Methods:
Androgen deprivation therapy with 6 months of luteinizing hormone-releasing hormone agonists (2 months neoadjuvant and 4 months concomitant and adjuvant) was given in patients presenting with 2 or more unfavorable clinical or histopathologic characteristics (≥T2c, Gleason 4+3, PSA >10 ng/mL, perineural invasion, and/or >1/3 of positive biopsies).
Note: to me, this is a bit more usage of ADT than I think is ideal - as a field I think we can dose escalate more and use less - but please note my stance on this topic is rather controversial - I’m drafting this in a longer discussion right now.
For today, recall CHIPP (Ref 2) used ADT basically 100% of the time to achieve 90% biochemical disease free survival. And between here and CHIPP, patients are quite similar (LR was 15% vs. 22 here and HR was 13% vs 15%). So this does appear to be less ADT usage and higher control so, from my vantage, likely more dose.
We’ve discussed kinetics at length on this Substack and here they report PSA kinetic data - for a second time, Yay!!:

This trial hits all the marks that I think are required to meet a 90% disease free survival in prostate cancer albeit with 45% ADT usage.
As I recommended one month ago reviewing our literature:
My back of the envelope calcs based on these studies and several others:
We should expect mean PSA<1 at one yr and <0.5 at 2 yrs for the treated cohort to exceed 90% bDFS WITHOUT ADT.
This should result in an ultimate cohort nadir around 0.3 or 0.2.
Read more on my thoughts on post-treatment kinetics here:

In this trial, using median - not mean and with ~45% receiving ADT, we meet these metrics and reach 92%-93% biochemical disease free survival.
This data is exactly the type of strong data with presentation of kinetics that will let us sort and verify which approaches are truly top tier. Again Kudos to the authors of the study.
Quibbles:
First off, we discussed previously the effects of duration of follow-up. Here we really do quite well. Basically 6.5 years of follow-up and they report 5 year results. Not perfect but in fact very strong follow-up. As we’ll review - this is consistent with the Ma data (ref 3), the FLAME-SIB data (ref 4) - both of which I think are very strong datasets. No issue.
Biochemical failure vs. all failures is a second known issue. On the plus side, as cure rates improve, this should be less and less of a factor. Generally it always lowers the cure rate to include clinical failures - even in FLAME which clearly presents both evaluations, the high dose arm drops 5% if and when you include any failure (much higher risk patient cohort but still illustrative of the issue). To me, this needs to be our standard - it is a drawback not to present it here. They do describe each failure - 8 total local failures, 1 nodal relapse, and 3 had developed metastatic disease, but I don’t understand this decision in our literature today - other than creating, at a minimum, a potential for significant upward bias in the results.
PACE - B (ref 5) appears to address this as I recommend. Here is the primary objective:
To determine whether prostate SBRT is non-inferior to conventional radiotherapy for freedom from biochemical/clinical failure in low/intermediate risk prostate cancer.
Yay! I wish that simple standard was… standard.
Beyond that ADT clearly impacts both biochemical relapse free survival and PSA kinetics in a direct fashion. If you look at the 7 year outcomes for the two arms, they demonstrate quite a few events with disease free survival falling to ~85% and 75% for the two arms (my estimation from the graph below).

As we have discussed, these numbers almost certainly will drop as follow-up increases to a median of 9 years. With longer follow-up, I’d anticipate at least another 3%-5% drop in these numbers putting them at 82 and 72. This then places this trial’s 7 year results in the upper 70s (say ~77%) for biochemical disease free survival. Maybe not, but I do believe that is most likely - these are Kaplan-Meier curves and not crude numbers, so yep, upper 70s is what I think this data says for 7 year outcomes.
Remember the highly cited meta-analysis estimates 7yr biochemical disease free survival of 93.7% with a lower bound confidence interval of 91.4% for SBRT. Even here with a great result relative to our literature and that analysis looks to be off by large magnitudes.
And you see hints of something similar in the kinetics with the once weekly arm showing the MEDIAN nadir beginning to rise (the red line rising between 4.5 and 5.5 years). This points to less than ideal control at a 5 year mark. (A heck of lot better than TULSA-PRO nadiring at the 3 month mark, but still.. (Discussed the TULSA procedure and data in prior post here))
In general, this later drop in the Kaplan-Meier curve is a bit inconsistent with other series that achieve 90%+ control. Generally, like in the Ma data or in the PATRIOT (ref 6) data, the curves remain quite high and stable if you reach >90% control at 5 years. This simply has more fall off than I would expect.
As an example, below is the Ma data - nearly identical follow-up at 71.9 months - looking their patient population by quartiles of PSA kinetics. Specifically this graph shows subsets by a ratio (PSA at 18mos / PSA at 6 months) - ie looking at rate of fall from 6 to 18 months to parse their outcomes. As you see below, even the 3rd quartile approaches 90% failure free survival at 7 years and the 4th quartile has a different shape than the above two curves to land again around the upper 70’s. So the worst quartile compares to overall trial result here - at least that is the closest curve. Remember, the Ma dataset is without ADT.

Here is the second example that helped to set my expectations: Flame SIB data - again nearly identical follow-up at 72 months. From the curve I approximate 87% vs. 73% for biochemical disease free survival and 80% vs. 70% for disease free survival at 7 years for the high and standard dose arms respectively. As a reminder, this trial has 84% high risk disease and 2/3rd received ADT.

To me, the 5 year 92% data in either the FLAME-SIB trial or the Ma data appear more robust than this trial - probably by at least a couple of percent. But really, we need more months of follow-up to really compare anything beyond 5 year results.
So realistically, I agree: these are quibbles and nitpicks. From a broad level this is really strong data and I think one must consider whether it raises the expectation for PACE B even if I think it is likely one step below FLAME-SIB or the Ma Consortium dataset.
A Broader Perspective:
This data is supported by the large Ma prospective cohort. It mirrors, in many ways, the results of the PATRIOT trial demonstrating excellent control. And it adds to the real possibility that the PACE B SBRT arm will outperform traditional fractionation approaches to ~78 Gy. To me, these studies begin to strongly argue that the alpha / beta for prostate cancer - at least when using our simple formula approach - is less 2 or less. Remember, this is quite a shift. Just a few years ago in 2019, the meta-analysis - our most cited dataset - used 2.5 and yet now only a few years later this appears to be significantly off target - because 2.5 would argue for ~85% biochemical disease free survival based on our literature as discussed below:

Based on my prior reviews of our literature, I have guessed 87.5 for PACE-B results. Here are the actual entry criteria for PACE-B - No ADT usage allowed
Low risk:
Gleason ≤ 6
Clinical stage T1-T2a
PSA < 10 ng/mlIntermediate risk: Any single criteria
Gleason 3+4
Clinical stage T2b or T2c
PSA 10-20 ng/ml
And for easy comparison, here is when the current trial added ADT - needed 2 of these factors to add ADT.
Risk factors for ADT in this trial:
>= T2c
Gleason 4+3
PSA > 10 ng/ml
PNI
>1/3 positive biopsies
I believe the low toxicity - it is lower dose SBRT and the urethra was spared to further reduce dose. Along with the smaller margins, that makes sense. I think this would be something I’d roll out in clinic quickly mirroring ADT per their recommendations.
This seems to clarify the bar for our specialty as well - we have a list of items when we might need ADT or higher dose and I’d suggest we focus on intent on that subset of higher risk disease and attempt to push doses higher for those patients in an attempt to reduce the need for ADT.
As the authors conclude:
Improvements in planning optimization and delivery techniques as well as use of intrafractional motion control systems are expected to further improve outcomes of SBRT treatments.
And if 92%-93%, creeps to 95% or above with better tracking / delivery, there really might not be a need for more dose. And that is from a guy who is biased and thinks dose matters.
Below is a post from just April 8th including a Twitter poll with small numbers that I included - I guess technically, I could have / should have known about this trial and fudged my number higher - but I’m not near perfect - I consider myself still learning. Here is what I wrote.
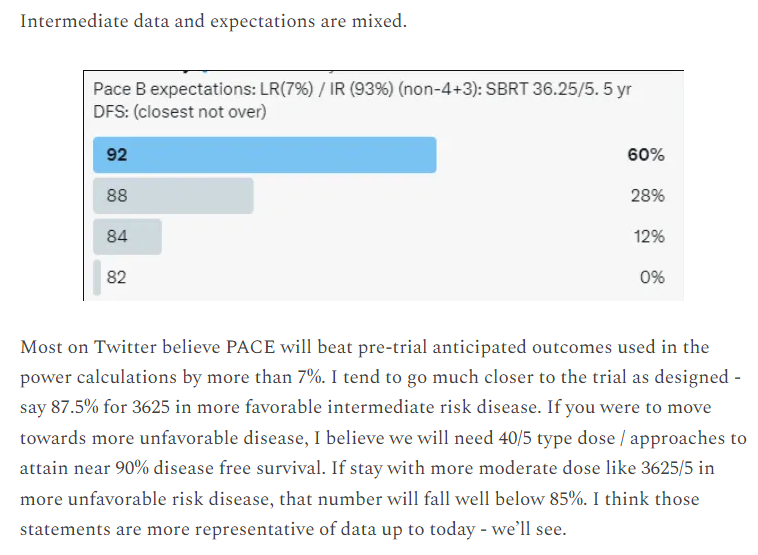
So perhaps I was too pessimistic. PACE-B eliminates ADT and that will clarify things a bit reporting clinical disease free rates as the primary metric. If between ADT and clinical vs biochemical disease free survival adds 3-5%, I’m still in the correct ballpark - again data is the answer.
And to me, that is why this data is important. I think it makes us consider pushing our expectations at least 2-3% higher. It is prospective multi-institutional data at ~92.5% biochemical disease free survival. So instead of 87.5%, I think one can argue that expectations of about 90% are a better estimate especially since 4+3 disease is excluded in PACE-B.
And therefore, as a trial that potentially changes expectations, it is an excellent trial to read in detail. Kudos to the authors!
For the record, I’m holding steady. I started to move towards 90% but based on ADT, kinetics, the shape of the Kaplan-Meier curve and the choice to present biochemical disease free survival, I still think PACE-B will demonstrate SBRT 3625 control below 90 leaving my 87.5% in play. But this makes that a bit of a gamble based me looking for nuance.
As always, the data will decide. Thanks for reading!
Looking ahead: An article on the horizon is to present the counter to the “dose matters” in prostate cancer. The counter to my discussion here is short term ADT is important even with dose escalation in intermediate risk prostate cancer. I don’t think they are actually that far apart. I think we’ve over simplified the ADT aspect a bit and I have some issues with the term “dose escalation”. Good to discuss both sides of the coin. I’m still not convinced the debate is settled while others might. As always, I’ll try to stay in the center and you can decide.
REFERENCES:
Every-Other-Day Versus Once-a-Week Urethra-Sparing Prostate Stereotactic Body Radiation Therapy: 5-Year Results of a Randomized Phase 2 Trial
https://www.redjournal.org/article/S0360-3016(23)00301-2/fulltextConventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial
https://pubmed.ncbi.nlm.nih.gov/27339115/Refining the definition of biochemical failure in the era of stereotactic body radiation therapy for prostate cancer: The Phoenix definition and beyond
https://pubmed.ncbi.nlm.nih.gov/34774650/Focal Boost to the Intraprostatic Tumor in External Beam Radiotherapy for Patients With Localized Prostate Cancer: Results From the FLAME Randomized Phase III Trial
https://pubmed.ncbi.nlm.nih.gov/33471548/PACE Trials (Intro should be required reading for residents pg: 10-21)
https://www.icr.ac.uk/media/docs/default-source/default-document-library/pace_protocol_v12_clean.pdf?sfvrsn=130f3069_0Accelerating prostate stereotactic ablative body radiotherapy: Efficacy and toxicity of a randomized phase II study of 11 versus 29 days overall treatment time (PATRIOT)
https://pubmed.ncbi.nlm.nih.gov/32416376/