


High Risk Prostate Cancer: Beyond FLAME and PRIME
Part 3 of my series on high risk prostate cancer: More trials to consider as we push for better.

MD Anderson just published high risk disease with 5 year outcomes of 86.1% using protons. They avoided pelvic treatment and still hit a very high number. And FLAME landed above 90% using an integrated boost with 84% of patients having high risk, again with local treatment only. Same time, across the globe in India, we hit 95% biochemical disease free survival adding in pelvic treatment along with ADT (90% DFS). Lots of options.
Recently, I saw these types of approaches bundled and labeled as “augmented” radiation - ie pretty much what I’ve been arguing for on this site. Honestly quite catchy and might work in today’s environment over my “give more dose” simplification.
But I’m not first - not really even close to it. Here is an editorial from Dr. Murthy from Tata Memorial in India published in July of 2022 - on the heals of the STAMPEDE data arguing basically the same thing. (Honestly, I had not seen this opinion piece until this past week or so).
Editorial - Let's Not Forget Local Treatment Intensification

So as we approach ASTRO, we’ll summarize a few trials to watch out for on the horizon and hopefully discuss a few interesting points along the way in what is, an exciting space.
To Refresh:
Part One of this series on High Risk diseases focused on the massive changes that ADT causes in the basic decision tree and we end looking at two views - one in favor of pelvic treatment and one opposed.
Part two focused on the FLAME and PRIME trials and the data supporting a generalized shift towards SBRT approaches in higher and higher risk disease.
And then two weeks ago we dove into a broad comparison look for intermediate risk disease attempting to correctly file the recent MD Anderson retrospective proton study. It’s an approach that appears to demonstrate great results up to High risk disease, while, to me, showing clear limitations in Very High Risk cancer.

PSMA staging effects: Will Rogers Phenomenon?
Maybe… but perhaps more complicated.
This topic is becoming a recurring theme but I see it as very important. We talked about it in our last article looking at the link between biochemical disease free survival and overall survival.
PSMA simply raised so many questions that one can’t answer looking backwards. We might see hints in the data, but nothing clearly in focus. This is simply a new test that is more sensitive and it changes things. Plain and simple.
Today’s standard, to me, is largely moving towards a POP-RT approach. More and more people I believe are treating pelvic nodes today than they did 5 years ago - at least in the higher end cohort of high risk patients. The results in that approach were strong and, amazingly, most men in that study actually were staged with a PSMA scan (that study began in 2011). In fact, maybe that is why the results are, if anything, better. On some level, perhaps we are upstaging prior “node negatives” to node positives - it serves to improve the outcomes of both subsets of patients.
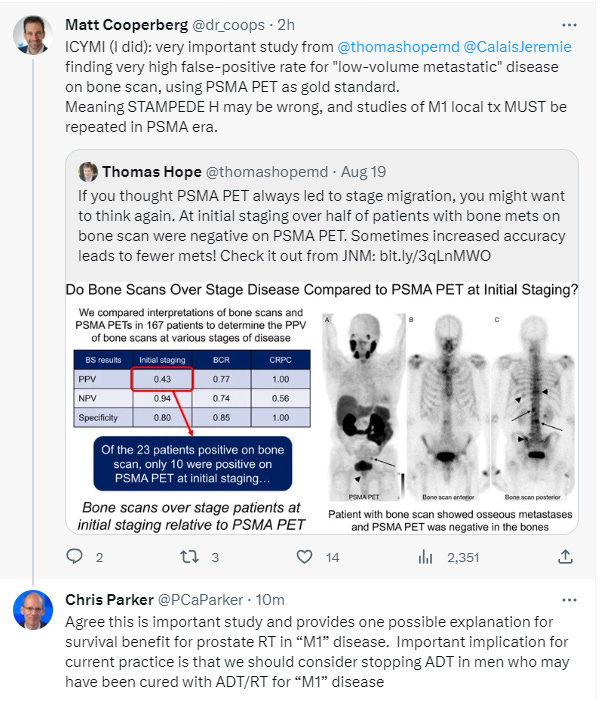
But maybe not just that simple for all metastatic spread. Within the last month, this intriguing study was published that ultimately lands with bone scans OVERCALLING disease. Many implications - too many to fully discuss today. Read below: very interesting post
But I still want to introduce the concept of stage migration as we shift to PSMA based staging.
Credit here goes to another great mentor: Patricia Eifel
Intermingled into most of her historical context lectures, but primarily on cervical cancer, she would discuss the Will Rogers phenomenon - a shift in outcomes where all stages have stronger outcomes with better staging.
- the Will Rogers phenomenon -
(Comedian from here who joked that when people opted to move from Oklahoma to California - Oklahoma got smarter. Cause, well, the ones that left for California weren’t the brightest and yet, at the same time California was smarter because they got some people from Oklahoma. This will happen with any new staging - here the node positive will be an “earlier” cohort and node negative will be even “earlier” - so both improve. Important concept to understand when looking across broad time periods and attempting to compare outcomes.)
The effect on our data from PSMA is going to be real and significant as it affects our ability to find lymph node disease and apparently changes what we believed was early bone metastatic disease, a topic we will return to in the future.
The Pelvis Debate Continues:
Context: I rarely treat the pelvis in a negative staged setting. Part of that is due to the fact that patients often are actively seeking protons and my pelvis option is tomotherapy based. Uniform scanning struggles to match IMRT for nodal coverage. So for some, yes. But mainly a VHR cohort.
POP-RT achieved 90% DFS and 95% biochemical disease free survival. I wish everyone just focused on DFS but I guess we can’t do meta-analysis that way due to lack of data so we’ve lowered our standards (my words). I think which number here is MOST compatible with the 86% for high risk men in the MDACC proton data would require the authors input. To compare staging practices and follow-up practices. How and when they scan or re-image? Frequency of follow-up? Maybe I can get the two of them to sit down together over a beer at ASTRO and discuss how they comparatively view the results… maybe.
But either way, POP-RT achieved great results and the addition of pelvic treatment likely adds benefit for many in this group. And I think that is why most are leaning more favorably towards pelvic treatment in their own practices - especially in the higher end risk of patients. Because even in the MDACC study with protons, one of the strongest results in publication, very high risk (US cohort of VHR) failed a bit over 30% with 7 years of follow-up. And while, more dose via SIB improved outcomes in FLAME, there likely is a role for pelvic treatment in some men with high risk and I’m more convinced in very high risk disease.
Consider the FLAME-SIB data (92% control) and suppose that 1 in 3 of the failures in that trial were due to treatable and curable nodal failures. In that scenario bDFS improves to 94%-95%. This is pretty much in line with POP RT whole pelvis approach so maybe the pelvic dose is sufficient to cure 1 in 3 nodal failures.
It is an interesting concept to consider. And seeing 94% in unfavorable risk disease fall to 68% in very high risk disease within the large MD proton series, I will likely be upping my pelvic treatment recommendations, at least a bit in higher risk men.
The March Towards SBRT:
And then ironically as we move to 5 fraction approaches, we drop the effective pelvic dose. Not a lot mind you but it is a 43.75 EQD2 at an alpha/beta of 2. If we only need 45 Gy to the pelvis, we are good. But if 50 Gy is really the stronger pelvic dose, then ironically, we are compromising that part of the treatment as we move towards shorter SBRT approaches.
PRIME though should answer this pretty firmly - its design is powerful in keeping 50Gy as the pelvic dose arm while using 25 Gy / 5 for the SBRT pelvic arm. If there is a difference in the pelvic dosing, it should show up in that trial. I trust data far more than a EQD2 calc.
And a Sunnybrook Phase I/II trial shown below pairs nicely with the PRIME trial. It will be interesting to look at the two datasets side by side. One offers far more dose-escalation to the primary - which should offset the minor dose reduction as the pelvic dose is dropped to 25 Gy in 5.
Below are slides from October of last year at our ASTRO meeting. Note: disease in this study is pushed to the upper 40s in 5 fractions to the area of disease.


I wasn’t present for the talk, but these are low nadirs and big doses in a very high volume center with decades of SBRT experience - consistent and believable within the context of other large published series. I worry about how broadly translatable this approach is across a variety of centers, but here, apparently it worked.
Should pelvic treatment trials include UIR disease?
I will say here that the MDACC data and the SBRT consortium data makes one really wonder whether the UIR group should receive any pelvic treatment in any trial. The extra volume comes with extra toxicity. (I’m aware of some data even going so far as to say - it doesn’t - but that is narrative (my opinion) - massive increases in volume lead to toxicity increases). And here is a new study, where this is documented in the form of pelvic fractures - pre-op rectal cancer yes, but fraction pelvic treatment:
Short-course preoperative radiotherapy increases pelvic fracture risk in rectal cancer

Conclusions
Every fifth patient treated with SCRT and rectal surgery presented with a PIF.
Every fifth patient had a pelvic fracture if treated with short course radiation - modern approaches - VMAT IMRT.
Again, shorter isn’t necessarily wrong, I just like to emphasize that it clearly reduces the margin between good outcomes and poor outcomes. So best understand details.
ACENDE-SBRT Trial:
And below at ESTRO this year Dr. Loblaw highlights the ACENDE-SBRT Trial - an SBRT boost compared to traditional fractionation with a brachytherapy boost.

Very interesting to note that low dose (my wording) NCCN recommended 60/20 really isn’t considered standard in this higher risk cohort while it remains the recommended path. I think most understand that we can push dose and if you look around closely, you’ll see this pretty consistently beneath the headline narrative of “just hypofractionate” that we see in our US guidelines.
And again, if SBRT, SIB, and protons get to 90% control at 5 years largely prior to PSMA scanning, should we really be looking a pelvic treatment in this cohort? I see less and less need, especially with improvements on the salvage side of treatment.
But kudos to the work done out of Sunnybrook! They have done great trials pushing forward along the SBRT with great outcomes. Highlighting this work was really a primary goal of this post today.
PSA Kinetics in High Risk:
As we’ve discussed, kinetics fall apart with ADT and certainly you can’t use non-ADT kinetics to assess a population that today - will all essentially require ADT.
A look at my database - 100 pts with ADT (mainly HR and VHR as the majority of UIR I’ll treat without ADT so this is a higher risk cohort than most US series).
In those 100 - 2 have failed. One at 24 months and one at 30 months. One significantly shortened ADT due to toxicity following good discussion and one had been managed conservatively for years and had a 1990s style prostate - massive local disease like the kind of stuff we saw prior to PSA. To date, with limited follow-up of less than 20 months, 2 of 100. One would be a Phoenix failure - both have clear disease on PSMA.
The other approach I’ve used is to assess whether patients achieve a nadir of 0.2 or less with 6 months - using this approach, I have 8 patients of the ~100 that did not reach that metric. If you tighten it up to 0.1 or less (based on a presentation at ASCO this year) about 15% did not achieve 0.1 or less at 6 months following treatment.
Maybe these really low 6 month post-treatment figures are meaningful, but I have much less confidence using any kinetics in the setting of ADT. I think it is an area of our literature / knowledge that would benefit from more data.
Other Trials on the Horizon:
First two lower risk studies just for context:
NRG-GU 005:
Honestly, not my favorite. To me, designed for an SBRT “victory”. Basically a verification of safety trial more than a head to head comparison of which is a superior approach.
Why do I say that? Well, margins in the hypofractionated arm are 8mm and 5mm posteriorly compared to 5mm and 3mm for SBRT. They treat IR risk disease with both a hypofractionated approach and a 5 fraction SBRT approach. The primary metric is….toxicity. With very different margins. Of course there are secondary items like disease free survival at 2 yrs - please, at 2 yrs? No difference HAS to be the outcome - honestly makes no sense to look at that metric that early. And entry criteria is a prostate<70 gm so it will exclude many straightforward hypofractionation cases - an important caveat to remember.
Later on, at 5 years, they will report metastatic disease free survival and biochemical disease free survival, but to me, this is clearly designed to show a clear “win” for SBRT in the short term and by the time 5 years rolls around, few will care. Doses and approaches will be different regardless and many will likely have moved on to 5 fraction approaches for even high risk disease - they won’t back track for LR and FIR disease. My opinion.
PACE B
The deeper I get into PACE-B, the more similar it is to GU-005 but has always seemed more balanced in approach from afar. It is a big dataset (874 men), and 5 year data is basically here today. (well in two weeks).
NOTE: in the SBRT arm, PTV and CTV doses are different
78 Gy / 39 or 62 Gy / 20 (standard arm) vs. 36.25 / 5 to PTV with 40/5 prescribed to the CTV.
“Dose heterogeneity was allowed within the SBRT targets such that maximum doses of more than 45 Gy were permitted” so this is not a cool plan - in fact a rather hot SBRT plan - even allowing a hot spot of 44Gy relative to 36.25 is over a 20% hot spot. So this is best considered an SIB approach to “CTV”. (I just recently noted this nuance - I thought it was more typical uniform dosing across PTV / CTV).
It includes favorable IR and LR patients:
Low Risk includes all of the following:
Clinical stage T1c – T2a
PSA <10 ng/ml
Gleason score ≤6
Intermediate Risk includes the presence of any of the following:
Clinical stage T2b-T2c
PSA 10 – 20 ng/ml
Gleason score 3+4
I want to return to this topic next week as results will now be presented in the plenary session at ASTRO.
PACE C
IR / HR disease - so the remainder of IR disease plus some HR disease graduates to PACE C. No pelvis treatment. Here all will get ADT.
60 Gy / 20 fractions vs. 36.25 / 5 fractions with 6 months ADT.
I haven’t dug this week here, but I assume the SBRT is similar with this really being a dose of 40Gy to the prostate despite a headline dose of 3625 cGy. The answer is found via the actual protocol - not the 70+ page design document - or we rely on the authors to report the dose differences in the articles.
Intermediate risk includes any one of the following:
MRI stage T2 (N0, M0-X)
PSA 10-20 ng/ml (prior to starting ADT)
Gleason 3+4 or Gleason 4+3
High risk includes 1-2 of the following:
MRI stage T3a (N0, M0)
PSA >20-30 ng/ml (prior to starting ADT)
Gleason 4+4 (and ≤50% cores positive)
* Patients will be ineligible for PACE-C if MRI stage T3a AND PSA >20-30ng/ml AND 4+4
No Gleason 5 disease. Goal again is 85% - non-inferiority a little tighter at 5% so 80% and up.
And remember this one relative to the new proton data…
This one will need to hit something up in the 90s to compete with the MD Anderson data we just reviewed. And if it falls short, the question remains open: are protons better or is the difference completely due to randomized prospective vs. retrospective analysis.
PRIME follows POP-RT
Following up on the success of the POP-RT trial (discussed in depth here), the PRIME trial looks to shift the standard to 5 fractions (discussed here). And ultimately, I think it will succeed demonstrating little risk for shortening treatment time to 5 treatment even in a high risk cohort.
POP-RT is a trial to know today and PRIME is a trial to watch for on the horizon.
As a reminder, here was the POP-RT criteria for pelvic treatment - again largely PSMA staged patients with an older, classic radiation risk assessment:
Roach formula Nodal risk >20%:
LNI risk (%) = 2/3 × PSA [(Gleason score − 6) × 10]
It would be an interesting question that will likely never be asked: can any “genetic” test demonstrate benefit over what was a simple old clinical formula. I personally love the old school simplicity in design.
Those are the main pieces I wanted to cover in high risk disease. A bit of a hodgepodge of information, but “high risk” represents a mixture of disease as well. We’ll see what ASTRO brings.
Ultimately, the data should lead us. The goal here is to follow that data. In the final release prior to PACE-B data, I’ll discuss what I’m going to be looking for in that study - well beneath the headlines.
As always, thank you sincerely for following along as we search for better. Now hundreds of subscribers and thousands of monthly reads. Thank you for the support.
PACE TRIAL DOCUMENT:
https://www.icr.ac.uk/media/docs/default-source/default-document-library/pace_protocol_v12_clean.pdf?sfvrsn=130f3069_0