
Approaching Singularity, Part III: Advice I'd Give My Younger Self
What the next decade likely rewards - directional ideas for individuals and our field.

In Part I, The Approaching Singularity - we set the stage - two converging singularities on a collision course. It’s a large picture view of our field looking at multi-decade trends in our field that will impact just about everything - from decisions on equipment, planning, staffing and our fields impact in oncology. This long arc of progress in radiation is towards a simple concept: Put more dose in the target and put less dose elsewhere - our Singularity so to speak. Today, that long directional arc is going to collide with an explosion in AI investment.
In Part II, The Approaching Singularity, we look at more specific examples and what this intersection might look like. We look at theranostics (Pluvicto), the new Reflexion treatment codes (billable at $3750 per fraction), CMS 2026 billing changes and consider how these “outside” issues pair with our own fields “Singularity.” Finally, I try to look at how these issues for our field will be magnified even further via the larger AI “Singularity” occurring beyond the walls of our field.
Today, we’ll move back inside the walls of our field and I’ll discuss how I would think about this type of information if I still had 10+ years ahead of me or if I were leading a program.
"I skate to where the puck is going to be, not where it has been"
Wayne Gretzky
In the rapidly changing world we are living in, hopefully you can now see the direction of the field and some of the larger external forces that will be at play. The goal today is to help on defining your path through / to that vision so you can successfully skate to where you need to be in five and ten years.
I love the field. I believe we create tremendous value in oncology. And I would recommend it today for those looking at career options. And yes, I believe that our field has strong trends towards simplification in ways, and that AI will accelerate those changes and add additional competition to when and where we add value.
Today’s article is what I might write for me if I were to time-travel backwards 15 or 20 years. I’ve learned quite a bit in some 30 years in the clinic and what I see on the horizon for the next ten years would make me adjust how I approached my career arc - not drastically different, but I would prioritize different aspects.
Maybe help one or two people navigate their careers one step more efficiently - that’s the goal anyway. I hope it applies to two main cohorts: people early in their career and to those more senior physicians who are helping to guide their programs or our field more broadly. As I said earlier, if we don’t become more active in the framing of our own singularity, pharma will define it for us.
Diversify:
If you’ve ever read the book “Rich Dad, Poor Dad”, as Radiation Oncologists - we are in the poor dad camp. If you’ve never read the book, “poor” refers to working for income within a non-asset-building professional archetype (i.e. too often - physicians).
Now realistically, we are blessed and very well compensated, and my career arc has been far higher than I ever would have guessed, but per the book, we are the poor dad.
A couple of quotes make this point:
"The poor and the middle class work for money. The rich have money work for them."
"If you work for money, you give the power to your employer. If money works for you, you keep the power and control it.", Robert Kiyosaki
The general premise is, if you have to go to work to earn money - that is an inferior path to owning assets that create wealth for you - while you are awake and asleep. Too often, physicians are income “rich” but must keep working due to a lack of wealth building assets - the money flows in from the work and flows out on stuff too quickly.
Further, he argues we are far too specialized. Even within medicine, we are specialized, but from his viewpoint, that specialization creates risk.
"The more specialized you become, the more you are trapped and dependent on that specialty.", Robert Kiyosaki
He suggests that the more specialized you become, the more you are trapped by that specialty. If your specific niche becomes obsolete or if you lose your job, you may find it difficult to pivot because your skill set is too narrow. I have no doubt this is true on some level.
Again, obviously I’m a Radiation Oncologist and I’ve had a great experience. But from today looking forward, I do think these are important messages if I am even 1/3rd correct on my thoughts for the volume of change we will see in the next 10 years.
What does Diversification look like in your job:
Here are six actionable items that I think create more diversification within a radiation oncology practice and thus, a bit more stability for you if things do progress more rapidly.
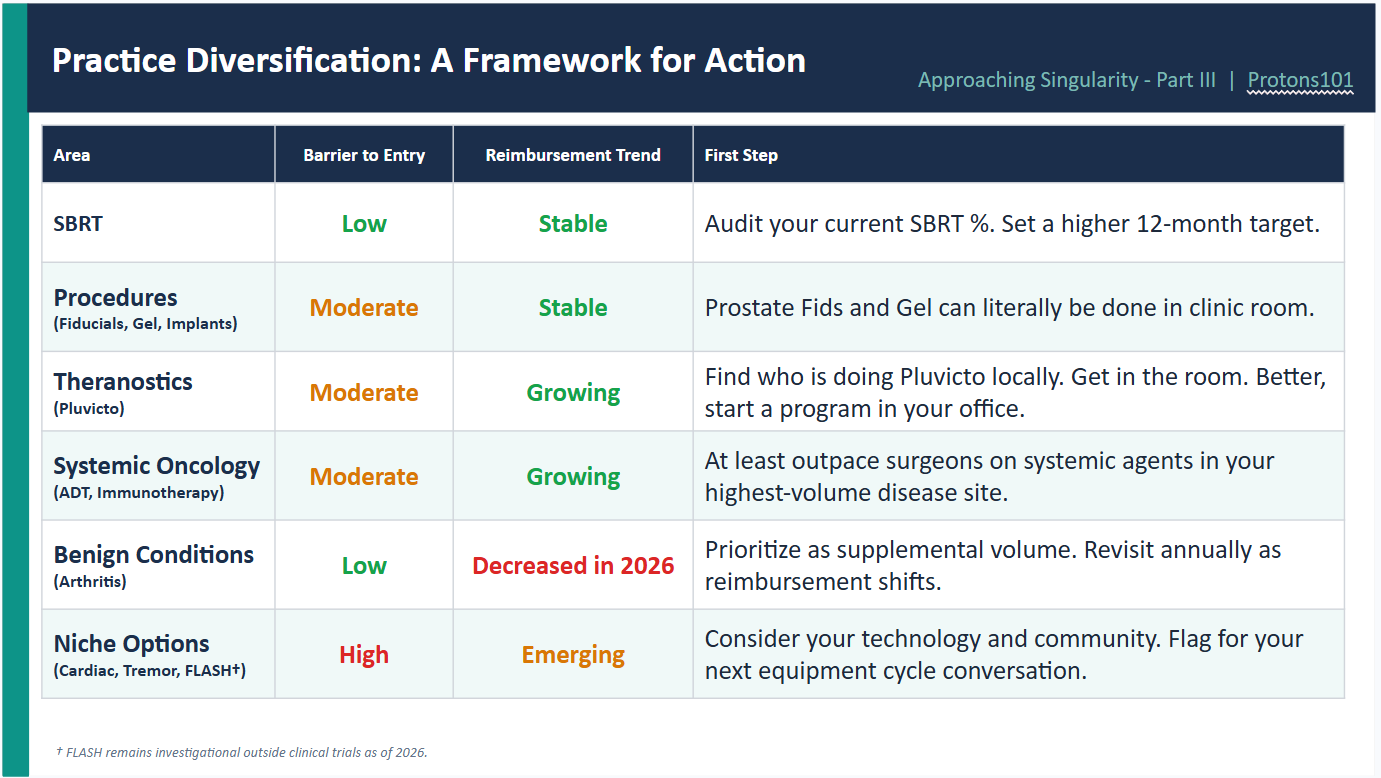
SBRT:
Drive SBRT in your region - again, I feel quite strongly that whatever percentage of your business today is SBRT, it will be a higher percentage and shorter in duration in just 3 years. Be the expert that people want to call.
From a daily “work” perspective, SBRT is one step busier - requires more volume, has more risk than say 6 weeks of radiation for lung or breast or 7 weeks of prostate treatment (all old examples), but this is where we are going. Payment is reasonable and I’d definitely focus on that aspect of practice.
Procedures:
Think fiducials or gel in prostate as entry level - try to go do them. I wouldn’t just funnel these to interventional radiology. Same with implants - these are niche items. For a while, we had enough revenue and stability within our system, that we could punt these things. Today, I’d be less willing (or be actively pushing myself to do more) to allow these to leave my reach. Keep your procedural skills high or improve them post-training.
Fids and gel placement for prostate cancer is entry bar - we literally have done these in an exam room. But I’ve been to meetings with radiation oncologists doing biopsies and fiducial placements for a variety of cancers. Interventional radiology is aggressive in pursuing these things - but they are often quite overwhelmed with volume - find your niche.
Theranostics:
Pluvicto is our current example that screams just how much opportunity there is in this developing branch of oncology. If you are not doing these treatments in your clinic, work on bringing them into your environment. We have the needed regulatory supervision covered. This expands your clinic “skill set” towards IVs / contrast / immunotherapy management - it aligns well with a direction of practice diversification.
Today, Pluvicto is gaining ground in an area that often overlaps our role in oligometastatic and high risk metastatic prostate cancer - despite external beam having great data in this area. Think about options for antigen specific delivered radiation for breast cancer where our data simply is poor.
Not only does it afford diversity via the treatment, but it keeps you in the center of the loop to help manage SBRT for the oligometastatic settings where you understand its appropriate value add indications.
Looking forward, I believe Pluvicto is going to be one of many of these types of treatments by year 2035. Don’t think of it as a one off prostate cancer treatment and let your department get passed by. It is a radiation treatment and you need to drive your local region.
Immunotherapy:
Especially if you specialize or see higher volume within some cancer diagnosis, I would want to control more of the drugs than we traditionally have done. For example, if you treat prostate cancer and you are letting Urology jump ahead of you in giving the new second generation ADTs - go get that business back. I understand this is might feel like a leap and can buck trends potentially with medical oncology, but if it is you or the surgeon looking at these options - certainly be ahead of the surgeon.
We have wide and deep oncology experience - back in the day some administered concurrent carboplatin. We have far more breadth of knowledge than many surgeons. For step one - at least outrace the surgeons. For step two - focus on your high volume patient cohorts and consider paths towards more systemic treatment integration into your practice.
Benign Disease: Arthritis
You see people actively doing this today - it is an easy way to diversify and physicians are having significant success in building up this aspect of their practice. It doesn’t require additional capital investment and it is safe, easy, low dose, and effective. I choose to list it later, because with the CMS reimbursement changes, it appears far less viable as a primary path today. To me, it will most commonly be a “filler” within the high capex framework - but it can serve as a bridge forward.
Specialized Radiation Procedures: Cardiac Ablation, Tremor, FLASH
A couple of more niche procedures might be reasonable to consider depending on your local setup. They require capital investment. I think very few radiation oncologists moving forward will hold the keys to decide purchasing paths so I put this one near the bottom, but they are ideas and areas to at least monitor and consider in your local area depending on your equipment options.
These are not going to be mainstream things in a “standard” clinic - at least for a good long while. That said, they offer a clear niche approach to broaden your practice.
Back in the day, I ran an 8 person practice. I kept my personal one-man clinic business line very simple - it was IMRT focused. I didn’t do procedures and I purposefully didn’t do SBRT - it slowed the machine down and we needed the full resource to treat 30-40 people per day in a small satellite.
Back then, the better business model was to consolidate procedures at a single facility in town and consolidate SBRT at the other large facility in town. And it made my life in a satellite easier at the same time. Most money was actually in the IMRT format - we split everything - but I did external beam - shifting to largely an IMRT practice with little else.
From 2005 to even 2015, that was viable. Today that would be too specialized - not diverse enough. It might work today but as fractions continue to compress, each year you have to be gaining market share moving from an old bar of 200 to 300 to 400 or more new patients annually per machine.
Within that landscape, I’d strongly recommend people in their 30’s do much broader treatments than just: “IMRT, external focused with a little SBRT on the side - no procedures - just old-school radiation practice”.
I really do think that if you look out more than a decade, you must continue to diversify and work on expanding your current skill sets. If you are in your 30’s today -to lead at age 50-60 - you’ll need to be doing a diverse spectrum of care.
Research: Consider the trends and gauge impact duration
If you are doing research, ask one hard question before you commit years to a project: will this still matter when it is time to publish?
Regulatory timelines, accrual curves, and publication lag mean a trial designed today may not report until 2031 or 2032. If the trends I’ve outlined in Parts I and II are even directionally correct, the clinical landscape that motivated your question may not exist by the time your answer arrives. That’s not cynicism — it’s basic career math.
Just this month, April 13th, Dr. Nina Sanford and Dr. David Sher published on the struggles for our field to confirm even Phase II trials (When Success Fails to Translate - JCO Oncol Pract). Only 17% progressed to Phase III trials and the median time for those to complete was 10 years. 10 years is simply not viable on any level today. Obviously our field demands Phase II and Phase III trials, but the more we consider where the puck will be and when it will get there, the better we’ll use our limited resources.
Just about seven years ago, I was pushing for a proton dosimetry based trial for high risk concurrent patients (details beyond today’s scope). Today, a close cousin of that concept remains in development. Problem is - seeing what I see today - the opportunity for the trial will largely be gone by 2030, well before trial completion. All of this is opinion, but I encourage everyone to strongly consider realistic perspectives in your choice of direction. New data will have to land in a shrinking time window.
From where I sit, it is not unwise to favor projects with shorter feedback loops, translational flexibility, or that directly address the transition points our field is navigating. A well-designed dosimetric or outcomes analysis that speaks to hypofractionation, theranostics, or AI-assisted planning might age better than many great “ideas” that do not consider and align with (or contradict) our approaching Singularity.
Financial, Part I: Know our Business
It’s hard to emphasize this enough - know the value of your work. Know the primary components that create that value. And then know the structure of how your facility / employer makes money within the world of oncology - start with radiation oncology as a focus but then broaden and consider radiology, interventional procedures, surgery, and then the beast that is medical oncology.
The better grasp you have of this - the more able you are to judge whether you are being compensated appropriately or not.
Think about this 400k x 30 years. $12M. You argue for 450k and it immediately moves to $13.5M.
This isn’t make-believe, in fact this under-sells opportunity - 450 vs. 400 is 12.5%. Back in the day, I re-negotiated our group’s contract. I moved the needle on compensation by over 60% knowing value. Sixty percent year over year increase (average of 4 years post vs. 4 years prior). This was via a third-party consultant working within non-profit setting setting a new five year value. I didn’t get money we should not have received, I got fair value for our value - for the first time in over a decade. The argument at the board and consultant level was market compensation for our work. Over the years, admin simply wasn’t keeping up with market. Know your value - know your contract - personally monitor and measure your metrics.
Understanding the business allowed me to reach financial independence a good 5-10 years earlier than if I had just kept my head down and focused on work. Today, if you only focus on work, the reality is - bluntly - someone is looking to undervalue your work to “apply” “your value” somewhere else. You have spent at least college plus med school plus residency creating value in your knowledge base and specialization - do not let some system syphon off that value via a one-way relationship.
What success looks like: Know your value. You know your work landscape and what you would prioritize. Last 4 years, I’ve worked part time - I believe it was a “fair deal” - far less income than previously in my career, but I thought it was fair and appropriate. The result: the job aligned better with my goals and value and despite significantly less income, I was probably happier than in prior decade related to work.
Success here is about appropriate compensation for the value you provide and making sure the overall framework aligns with your personal goals.
Finally as brief financial career advice - acquire assets early - don’t just rely on working for income. Assets compound. I used mainly stocks, along with occasional real estate and one crazy small venture into a proton center (not recommended). Eventually, these create momentum that really can generate incredible flexibility. Again, the “Rich Dad” has money work for them.
Summary:
We are sitting in a great field with the ability to have tremendous impact with oncology. AI is going to accelerate change - everywhere for everyone. Success, on some level, will be more dependent on your ability to change and adapt than it has been at any point in the past.
To me, there are clear steps to take - even well within the framework of “radiation oncology” - that will provide far more stability and flexibility within this type of environment. Am I certain these avenues are required? Of course not, but even if you decide to stay focused on just an external beam practice, I feel quite confident that watching and following these “field-adjacent items” will make you better at your primary path. If that is “worst-case”, then I think we have done well.
I’d like to block one visit per quarter (maybe 2) moving forward to visit programs within a visiting professor type framework. The goal is help educate the next generation of experts - to pass along information best I can. If you have interest, reach out. Below is a direct email link:
Agreed w all except gel. Use the AVOID technique and just don't do it. Maybe the biodegradable balloons will pass muster and eliminate most of the risk, then... OK. Sure.