
Protons 101: The COMPARRE Trial - Proton vs. IMRT for Prostate Cancer
Has the opportunity for protons to demonstrate superiority in prostate cancer passed?

As always, author of one: if you see an omission or think I missed something, please reach out or comment below.
Background: I’ve now got about 4 years of experience at a large multi-room proton facility. I’ve been involved with brachy since back in the 90’s. Worked on rectal toxicity for the original dose escalation trial of 78 vs 70 back at MDACC. Over the decades, I’ve done quite a bit of work in prostate cancer..
Today, we will review the COMPARRE Trial (ref 1). I want to start by saying Kudos to the team at the University of Florida for pushing for and working so hard on this trial! They have been leaders in the field. I have mirrored my hypofractionation practice after their long-term outcome studies (ref 2) and I have been very impressed with both the excellent PSA kinetics post treatment and very limited toxicity profile of the approach. I truly believe they have demonstrated a top tier approach for the treatment of prostate cancer.
But here, I’m going to document why I believe the COMPARREtrial is too little, too late from the perspective of the proton industry. The trial will fail to show any biochemical PSA difference and due to a combination of factors, it will be viewed as a negative trial - even if the primary outcome is positive. Here is my rationale.
The COMPARRE TRIAL:
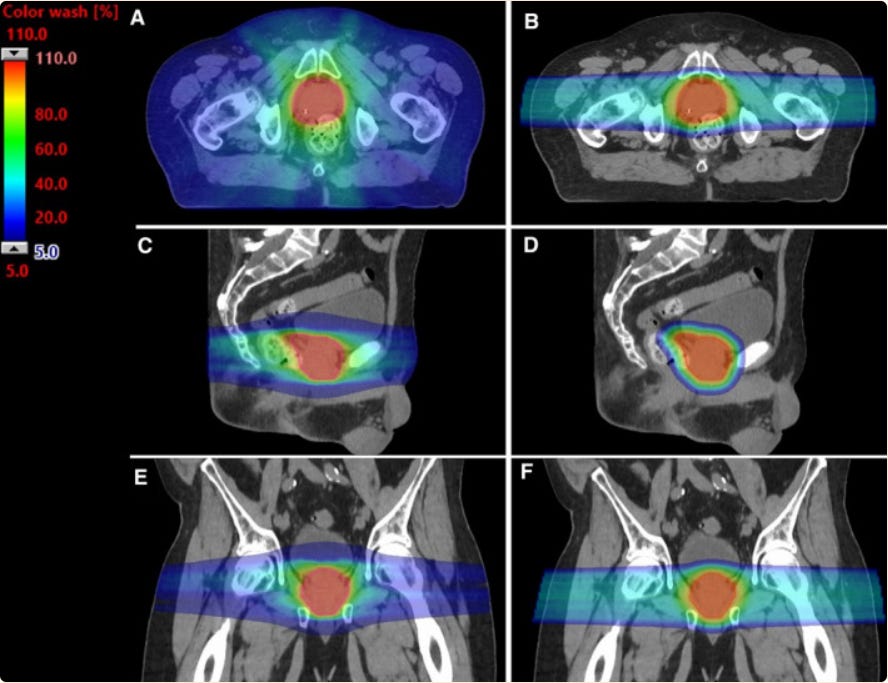
Trial will enroll 3000 patients. It is prospective but not randomized. It includes both “traditional fractionation” 78 Gy / 39 fx and “hypofractionated” 60 Gy / 20 fractions. It enrolls very low to high risk (excludes very high risk) patients and subgroup analysis are planned across a variety of outcomes. It looks to determine, in simple terms, whether the differences in image above matter to clinically measurable outcomes.
It is a large scale trial - 56 study locations and accrual of 3000 patients. It is and will be important data on some level. It is scheduled to be completed by 2026.
Primary outcome is bowel urgency and frequency via EPIC at 2 yrs. This makes sense. If you read my article on OAR metrics (OAR metrics demonstrating correlation to clinical outcomes), arguably changes in rectal toxicity are some of the most reproducible outcome findings that have been show with dosimetry improvements. If there is any improvement, this metric has potential to demonstrate a difference.
It includes 3 secondary metrics:
Gr2 or higher toxicity events using CTCAE 5.0 (at 2yrs) (appears to be a combination event - ie not single site, simply cumulative Gr2 events.)
Gr2 or higher patient toxicity events using PRO-CTCAE (at 2yrs)
Biochemical progression using Phoenix definition at 3 yrs - 2ng/ml high than nadir
It is a straightforward trial and uses very standardized outcomes. Rectal/Bowel changes as the primary outcome makes sense.
Is this trial too little, too late?
The “Glorious Upside”
First, lets look at the positive side ceiling for the study. Primary endpoint shows a reduction an improvement in EPIC toxicity and the secondary endpoints of higher toxicity for bowel and even bladder are a bit improved.
In today’s world, this should be a difference of mild toxicities. Gr3 complications are infrequent. So in this “winning” scenario, we see a slight reduction of Gr2 and Gr1 toxicities on both patient and physician related events.
That is the glorious upside for the trial from my perspective.
The odds that at 3 yrs there is a difference in cancer control via Phoenix definition outcomes approaches zero.
Here’s my rational. I track my own outcomes on spreadsheets - have done so for decades - generally one site at a time - current project is prostate cancers. Currently I have over 200 patients with decent follow-up - there is one Phoenix definition failure on my spreadsheet today. I’ve been here 4 years (spreadsheet updated almost daily). I have a second patient who had a positive PSMA (but didn’t fail Phoenix def) and I have handful that might fail or might be bounces (we’ll know in the next 12-24 months). Those are the events. (And the single Phoenix definition failure had a PSA >60 and refused ADT).
Simply, it is far too early in a highly successful treatment (read as any high quality radiation approach) to use Phoenix to look for differences in outcomes at 3 yrs outside of high/very high risk only patients. No wonder everything in prostate cancer using “non-inferiority” studies “proves” “non-inferiority”. Like I’ve said previously, per NCCN you can do any number of fractions to any dose as “standard of care” and this is why - we don’t even seem to look for differences.
In fact, with PSMA now available, I think it is possible that most failures will be radiographically diagnosed in the trial. Results might depend on how the trial “influences” physicians to order PSMAs. Patients in the PBT arm, I presume, will mandate earlier PSMA scans, while you can argue that physicians might influence outcomes by waiting for 2 mg rises over nadir. (In my personal practice, I start looking prior to that for many cases, once a rising PSA pattern clearly arises.)
I’ve argued for years, we should be using % of patients reaching 0.2 at 2 yrs (or something similar) to help determine the BEST treatment fractionation approaches for obtaining LRC. Using this type of PSA kinetic information, I think there would a chance to see a difference in LRC outcomes in this trial, but as written. Near zero. Results will be the same. And if they are different, confounding via imaging differences will be an issue of discussion - it is prospective, not randomized.
(Note: I understand the issues linking PSA to clinical outcomes - maybe a different post for a different time, but today I needed to explain why bDFS in this trial using Phoenix definition will be no different).
So the primary toxicity endpoint is positive. Here is what we would have:
A reduction in minor toxicities.
And the naysayers will rightfully point to the following:
We’ve moved on. Beyond this trial, we have “proven” that rectal spacing decreases GI toxicity (see my prior rectal spacing article for rationale for quotes), many modern trials report zero or one total Gr3 toxicity events (think MIRAGE (ref 3) or Barrigel (ref 4) trial). And on the outcome side, we have proven that using approaches like ASCENDE-RT (ref 5)or the FLAME SIB (ref 6) approach that we can push doses far higher while improving bDFS with still quite limited toxicity. And further, SBRT data continues to evolve that demonstrates that in the hands of some we can do SIB SBRT down to as little as 2 fractions to advance treatment outcomes with rather minor toxicity risks compared to more traditional approaches.
Each and every one of those arguments are very valid.
That means the window for a victory would be to argue 1) really strong LRC (albeit never measured against “the new standards” of brachy boost or to SIB dosing schedules) paired with 2) really low toxicity. Essentially a “good enough” argument on the cure side while minimizing toxicity risks. (if you’ve read the blog, I’m not a huge fan of these types of arguments)
For prostate, I don’t think that is a bad clinical outcome to favor. It just isn’t what proton therapy needs to achieve on a broader industry level. Prostate cancer today IS a balancing act of toxicity risk vs. LRC failure risk which then can result in further treatment. And realistically, even worse, is that I think this type of argument ONLY holds up if other trials from other sites have clearly demonstrated that dosimetry differences from proton plans impact clinical outcomes.
Ironically for me, if being truthful - I’d actually pick a compromise and go for “good enough” for prostate cancer treatment. I wouldn’t use ADT for my prostate cancer in many situations where it is considered “SoC” - they have terrible toxicity and I understand the risks of avoidance (mainly UIR or number of biopsy cases or clinical HR low Decipher cases). I’ve done uniform dose SBRT and, at least in my hands, I do not believe it is the optimal approach (different topic, different day). I’d go with the approach I use in my clinic, the UFPT approach per the reference, and try to get to 7yr bDFS of 90% or so with really, really low toxicity risk and I doubt I’d push harder on the first line treatment.
My PBT Experience
In my practice career, I moved from an IMRT environment to a PBT environment. Here is what I *think* I’ve seen: I think I see less minor bowel bother - it has essentially gone away - it was always mild and required pretty good patient questioning to find but not uncommon, but now it is very near zero (couple of percent) range - the difference has been noticeable and consistent with this data out of the Mayo Clinic from 2020 (ref 7)
From the Mayo abstract: (BF, bowel function)
In the BF domain, the IMRT cohort experienced greater decrement (−13.0 vs −6.7, P < .01), and had a higher proportion of patients with clinically meaningful reduction (58.4% vs 39.5%, P = .01), compared to PBT. At 3 months post‐radiotherapy, the IMRT group had significant and clinically meaningful worsening of BF (−9.3, P < .001), whereas the change in BF score of the PBT cohort was no longer significant or clinically meaningful (−1.2, P = .25). There were no significant or clinically meaningful changes in UO or UI 3 months post‐radiotherapy.
(I continue to say, I don’t know if this due to me seeing far more volume of patients per year, a dedicated prostate treatment room, rectal spacing, or protons - it likely is a combination of all of the above.)
Secondly in my experience, PSA kinetics post treatment are different between IMRT and PBT. I’ve given a reference (ref 8) but you can likely find any answer you want these days - I’d say we have no great data. But, I’ve done brachy, IMRT and now protons. My PBT PSA kinetics seem more comparable to brachy than IMRT. In IMRT I did not warn of the bounce, here I do and here it comes early - like 6 months. It seems different. And I think that supports a possible difference in local control rates.
Third, I really like the 7250 cGy(RBE) in 29 fraction approach per Florida with a reduction at 6000 cGy(RBE). Bladder toxicity might be a touch more than 2Gy/fx but I’m not even sure there. PSA falls quickly and nadirs low - in my experience lower than what I saw 5 yrs ago. No data, just opinion. Of course, I now SIB any definable lesion with IMRT so they would likely nadir lower as well.
PACE-A and a different perspective
But here is a different thought as to how one might measure the opportunity for our field more broadly. PACE-A was just presented Feb 13th at ASCO (ref 9). It is a trial looking at SBRT 36.25/5 fractions to surgery (so relatively LOW dose on the SBRT side - MIRAGE had an SIB option to 42.5 / 5 as just one example). In this study we see improvements in urinary incontinence and EPIC sexual function but a significant increase in patient reported moderate/big problem with bowel symptoms.
So in that light here is the opportunity for radiation oncology - show a significant reduction approaching 1%-2% in bowel toxicity which then fundamentally makes the option between radiation and surgery different as surgery loses one of its main advantages.
With surgery, you always will have the procedure and downtime. PACE-A shows continued risks for urinary and sexual function.
Radiation would then offer two approaches.
A short quick SBRT approach where you risk bowel issues that are not insignificant for some but gain on urinary and sexual health vs surgery and the process is completed quickly.
A longer hypofractionated course (perhaps with protons) which nearly negates any bowel difference, leaving the RISK of this approach as simple as the 4-6 wks of time for daily 15 min treatments with defined GAINS in urinary and sexual health and avoidance of a large procedure.
Finally, as a large prospective dataset, we will see more information regarding 2 Gy vs. 3 Gy per day fractionation from a toxicity standpoint. I just don’t believe that analysis will benefit the proton industry but it may offer good insight into expectations that we see today for these two fractionation schedules in the US. Prospective data is always good.
I think that frames the upside for the trial for both protons and for field more broadly from my perspective.
The downside: Primary endpoint shows no difference
And if the primary endpoint shows no difference, along side what I predict to be no difference in bDFS, this trial will be a major negative. It will be listed along side of the uniform scanning lung trial and it will be a very valid argument against the proton industry in the treatment of prostate cancer, especially in the setting of uniform dosing. (Goal here is to call balls and strikes.)
As I’m slowly describing here in this Substack, protons must demonstrate a “big win.” I don’t see this trial as having any real opportunity to demonstrate that type of difference. It is estimated to be completed in 2026 and in many situations, the standard will already have iterated and progressed.
Years ago was the better opportunity to demonstrate improvement using protons. IMRT has progressed quickly as outlined above. This study is simply 10-15 yrs late to the table and the bar to show clear improvements over IMRT has been raised significantly - which is good for our patients. I do think it had greater opportunity in prostate cancer around that time, not saying one or the other, but the opportunity was then more so than now.
This history reminds me of Cyberknife. I think, back in the day with the tracking and an integrated SBRT approach, it had a real advantage. Yet, no randomized trials were performed and today, MRidian tracks with arguably better imaging and certainly no fiducials needed. The opportunity to demonstrate superiority is in the history books for that machine from my perspective. This trial will help determine whether that analogy holds true for protons and prostate cancer.
One final comment: Across various sites, I think protons hold potential for improvement and I firmly believe we must fight for better. I do believe in the next 5 years we’ll see stronger data supporting use, largely at other disease sites. That said, the goal is improve cancer patients outcomes - more cancer cures with less toxicity. And if we do that with or without protons, I’m good.
REFERENCES:
Prostate Cancer COMPPARE Trial:
https://clinicaltrials.gov/ct2/show/NCT03561220Five- and seven-year outcomes for image-guided moderately accelerated hypofractionated proton therapy for prostate cancer
https://pubmed.ncbi.nlm.nih.gov/34965846/Magnetic Resonance Imaging–Guided vs Computed Tomography–Guided Stereotactic Body Radiotherapy for Prostate Cancer The MIRAGE Randomized Clinical Trial
https://jamanetwork.com/journals/jamaoncology/fullarticle/2800541Hyaluronic Acid Spacer for Hypofractionated Prostate Radiation Therapy A Randomized Clinical Trial
https://jamanetwork.com/journals/jamaoncology/fullarticle/2801296An Updated Analysis of Survival Endpoints for ASCENDE-RT, a Randomized Trial Comparing a Low-Dose-Rate Brachytherapy Boost to a Dose-Escalated External Beam Boost for High- and Intermediate-risk Prostate Cancer
https://www.redjournal.org/article/S0360-3016(20)33613-0/fulltextFocal Boost to the Intraprostatic Tumor in External Beam Radiotherapy for Patients With Localized Prostate Cancer: Results From the FLAME Randomized Phase III Trial
https://pubmed.ncbi.nlm.nih.gov/33471548/Comparing bowel and urinary domains of patient-reported quality of life at the end of and 3 months post radiotherapy between intensity-modulated radiotherapy and proton beam therapy for clinically localized prostate cancer
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7643652/Characteristics of PSA Bounce after Radiotherapy for Prostate Cancer: A Meta-Analysis
https://www.mdpi.com/2072-6694/12/8/2180PACE-A: Abstract #298, ASCO Genitourinary Cancer Symposium 2023, Initial Release Feb 13th, 2023. Lead Author: Nicholas J. Van As et al.
https://meetings.asco.org/abstracts-presentations/217340