
The World According to Timmerman...
Well, at least his views from a recent talk and a recent podcast.

At ASTRO, I sat front row for a discussion regarding prostate cancer treatment (so excuse the angle). And in the talk, amongst true leaders in the field, Bob Timmerman threw this slide up…
“giving more than 5 treatments (for prostate cancer) is OUTRAGEOUS in 2023.”
It is like when when a Twitter / X post lands on a slide. I’ve met him twice - once right after the talk and once many years ago. And ironically, we’ll begin today with:
I don’t agree with the slide.
I’ve been in rural Arkansas for decades (with really good equipment) and I just don’t think we should abandon fractionated treatment options for prostate cancer. I think it has higher toxicity (granted, mild) and many physicians just don’t have the volume / expertise to jump. We’re closer now that PACE-B has been presented but this slide was actually 2 days prior to that release. I mentally wrote it down and took a picture - I didn’t love it, but it is what it is and I figured somehow I’d work it into some future discussion.
So about 3 weeks after the meeting I was going for a jog and needed something to listen to and, if I’m being honest, quite oddly, I put on a radiation podcast to exercise to. Go figure.
The podcast was from the Accelerators Podcast and the main invite Dr. Timmerman. As I left the driveway I thought to myself, “well, this will be interesting.”
45 minutes later, I returned home really amazed at the story I had heard. Today is what I think I heard. Hope you enjoy.
Note: Today is MY context of his words and the podcast. Blue block quotes are directly from the print article, italic quotes are verbatim from the podcast and much in the middle is my paraphrasing of his main points.
The Accelerators Podcast - Dr. Timmerman and Dr. Sanford
To me, the goal of this Substack is to cover important topics in radiation oncology. Can’t get to all of them obviously, but help keep people up to speed with some important events. And even though this podcast is beyond traditional media (much like my effort here), it is something that every radiation oncologist should hear in my assessment. Especially the first 30 min which were very clinically focused - to me are amazing. Strong enough that today, we’ll attempt to blend three items: that podcast, his 2022 story of the Timmerman tables, and notes from call between Dr. Timmerman and Dr. Jeff Ryckman into a tale of sorts. And so we begin.
Just to back up, this is the physician that basically self-created a table of normal tissue limits for short / high-dose treatments (SABR / SBRT / SRS). It basically IS the reference document. And so the discussion was literally with one of the main people to move the needle forward for our field - helping, amongst many other many talented physicians across the country and globe like Lax and Blomgren (ref 1,2) make the shift towards shorter and shorter treatment approaches (maybe a different tale on a different day).

But regardless, he was an early adopter and certainly in the US, has been near the center of that progress regardless of perspective. Here is a link to his version of part of that history - apparently the most downloaded Red Journal article of 2022:
A Story of Hypofractionation and the Table on the Wall
It begins….
I was recently informed that I won a contest that I did not actually enter. A Twitter poll was organized through @Radiation Nation inspired by Sue Yom, the new editor of the journal, asking, “What do people consider the gold standard for treatment planning for hypofractionated RT?” Response options were “HyTEC; AAPM TG-101; Timmerman Sheet; and NRG/RTOG protocols.” With just over 100 total votes in 24 hours, “Timmerman Sheet,” which at University of Texas Southwestern we call our “constraint tables,” won with 37.5% of votes. Not to rub it in, but 2 of the other options, “AAPM TG-101” and most “NRG/RTOG protocols,” were taken directly from older versions of our tables.
And the podcast really starts with a bang as well.
“We had one of the.. the second Cyberknife in US or third. In fact when it first came, it didn’t even have a planning system so it sat quite a while because people thought it was a good idea to have system before you use a machine.”
Like I said, he has done this for a while and speaks in a very natural and straightforward manner which makes it a great story so many of the words below are his. The first question talks about his career spanning from 2D to SABR to Flash and beyond, with the question coming down to risk. Basically asking if our specialty is simply too cautious and it lead to a number of great answers. Again, simply great insight from a leader in the field that is littered with great radiation oncology quotes:
The Shift was Measured:
He walks through that he didn’t see his path as having much risk, although it still ended up making him nervous at times. It was measured and proceeded scientifically according to measured toxicity.
He started with the tale of these early SBRT type approaches beginning with the treatment of metastasis in the liver and describes that at the time “all the giants in radiotherapy that heard about it at the time said this is crazy, shouldn’t be done. And that there will be horrible late effects that could occur in those patients if they live long enough.” So then we moved to lung - thinking early stage lung cancer could live longer than the metastatic cases and basically, answer the late effect question. They started at a dose of 8Gy x 3. Still quite a high dose. (This was around 1998).
He then continues, “we hit 14 Gy x 3 for, this is again early stage lung cancer…. Anyway 14 Gy x3 and I got chicken. I wanted to stop the escalation. But in the grant that we wrote to do that trial we said our goal was to find the MTD - the maximum tolerated dose. So I called the NIH where the grant came from and the program officer told me he’d get back to me. And when he called back two days later he said, “we paid you to find the MTD, now go find the MTD.”
Simply a great story - ultimately in 5-7cm tumors the MTD was reached: 24 Gy x 3. An amazing accomplishment that pushed the cure rate for this disease from poor (my words) - say 20% or less for 60Gy in 30 fractions via a “postage stamp” approach to 95% local control using these new ablative doses. As he acknowledges, pushing the dose beyond what is likely required for many smaller lung tumors. (NOTE: this is old enough data that this is in a homogeneous lung calc setting so closer to 20-22 Gy per fraction in today’s heterogeneous world - I mean you come here for details).
“That’s first base for beating cancer right? You gotta get the tumor that you see gone and it was 95% effective at that.”
But historically, in my assessment, we have often been limited by both our history and technology and so for many reasons, we couldn’t get there. And we rationalized it by just looking at the toxicity side of the equation. Or as he stated:
“We didn’t sort of take blame for local failures as a toxicity in a sense that there’s nothing worse for those patients both in terms of their outlook of life as well as physical side effects that they get from tumor recurrence. Tumor recurrence is a terrible thing to have happen to a human being. And so I think that… All of us should be trying to improve our numbers if they’re not 95% and in many things in the field its not. That said, we can’t be caviler about toxicity.”
As I’ve said repeatedly here, today I believe we confuse shorter with better. But as I’ve written, SBRT is great, not because it is shorter, but precisely because it massively shifted expectations for cure. It wasn’t “about the same” or “close enough” - local failures dropped 16 fold. Read that again. From 8 out of 10 to 0.5 out of 10. That is why I keep the two concepts separate: shorter vs. better. Maybe I’m just old enough to remember this shift and it grants more context. In the late 90’s I was in training and so I literally lived through this era.
We Fractionate to Avoid Late Toxicity - We Thought.
And then there was this very simple explanation for fractionation - a great nugget - stated more clearly than I have heard it explained answering the “why?” as to why the other leaders were so scared to move in this direction.
“Late effects are the reason for fractionation. If it weren’t for late effects, there would be no fractionation and 2 Gy per fraction was extreme end of the spectrum to deal with late effects. And it pretty much eliminated late effects. But from the get go, we knew that 2 Gy per fraction is not as good against tumors.”
He basically described that using this dose, you could treat an excessively big target and, my words, just get away it. And in fact as his data matured in lung he stated he was surprised at the lack of any real late toxicity. Which leads to the next theme - either the surrounding tissue was not needed or it healed. So long as one of those two items occur, the patient recovers.
SABR, the ultimate hypofractionated threat to conventional radiation therapy, emerged in the mid-1990s via a variety of independent experiences from across the world. All, however, derived from very dramatic improvements in technology, technology that Kaplan, Fletcher, Lampe, and Bushke could hardly have conceived. Rather than exploit the biological elegance of differential repair, SABR simply used technology to compartmentalize tumor from normal tissue.
Note, another theme from this Substack emerges - technology. We do what we do today because of technology. We are a technology based field.
The SBRT Era: How His Tables were Interpreted:
“At that time there were a number of centers publishing SBRT type work in lung cancer and it just sounded magic. It seemed like every tumor was controlled. Nobody had a side effect. Nah.. …That’s like immunotherapy right? When immunotherapy was first in all these checkpoint this or that trials that were published in the New England Journal, you know improvements in survival, no side effects. …I think that’s a scandal in itself, I mean the way those things get reported in those high profile journals.”
I laugh as another topic of this site landed - there are narratives in medical literature. You need to be aware of the current narrative and the “path of least resistance” to progress within the academic structure of the moment. Good to see this point made and we return to it below.
“To that end I think that we have to re-look at this. I did put out toxicity tables that people have used to be safe or be as safe as they can and I gotta tell you how I used them all these years and I didn’t realize I was using them differently than everybody else. … I have never used them as a line that you shall not cross.”
Planning goals: (basically in order of priority)
You obey the spinal cord constraint
(people simply do not comprehend this risk appropriately)Treat the tumor / cover it fully
(Most of the time we do it, have to treat it, to cure it)Have very steep dose gradients
(the initial priority of his program - constraints came later)Respect normal tissue constraints
(because if you can keep risk low, why not.)
“So almost every patient that I’ve treated, if it was next to something, I exceed the constraint of that thing. I did that all the time, thought everyone was too. Then it came to my awareness recently that people were making those hard stops.”
We simply created compact dose distributions with isotropic falloff.
Again, I think nearly everyone will learn something today - if not you, at least now you have a document from the MD behind the table that you likely use to show to your physicist team or dosimetry team or administrative team. I guarantee you someone has put the breaks on things that deviate significantly from this approach based on red vs. green checklists on a plan document.
“I treat brain tumors, that was my chosen specialty”:
In the brain, like other structures, there is a sigmoid dose response curve - ie there are low doses where nothing happens, and then stuff starts to happen, and then all have necrosis.
Then he gave a great CNS example - doses relative to treatment of normal brain - reasonable sized volume ~2cm target volume: (clearly volume / dose dependent as he notes, but the basic curve looks like this:
At 12 Gy the curve begins (say 5% risk) - some toxicity begins to show.
14 Gy - half the people ended up with this “explosion hole in their brain that you wouldn’t believe”.
At 16 Gy - it was 100%.
“The difference between the brain and below the neck is that the brain doesn’t heal very well. You know you can give 20 Gy in 1 to a brain tumor but you can give 20 Gy THREE TIMES! to a lung tumor and not have bad toxicity.”
Do we count toxicities more than other fields?
Damage vs. Damage that “won’t heal”
A few great quotes as an intro to this topic. Quite relevant in today’s world.
“Most of the time we’re mopping up after surgery so they don’t want much toxicity from that and so you give small daily doses and you give big volumes ‘cause your not quite sure where it is going to recur.”
But at the other end of the spectrum are the ablative cases, where either surgery or radiation approaches carry risk. The cancer is simply in a tough place and either way there is toxicity risk. Instead of arguing the SBRT is “better” or vise versa, he argues to put the patient at the center of your discussion with other specialties and approach it from this position: here are the problems if I treat and there is a 5% chance that I’ll create damage that “won’t heal”. Often from that position, the discussion proceeds better.
And then he returns to the “won’t heal” part of the damage statement describing it like this:
“Surgery is a great treatment. Cures more cancer than any other treatment by far. But there are times when ours is far more elegant…. Surgeons injure patients every time they operate. It’s a trauma. If you did that to someone on the street, you’d be in jail. So they injure everyone they treat and yet, it heals.”
As the beam gets smaller and we have more precise technology, “our therapy is getting more and more like a knife.” And a knife creates a wound that can heal - this is basically the shift we are seeing in our field.
And he gives a great example of priorities - simplifying the task from my view. If the goal is to cover the tumor, then you need to look really closely at the tissue nearby. And that seems to have been his approach. Cover the tumor with rapid fall off.
And if you think about adaptive workflows which prioritize the 2cm ring of tissue just beyond the target (often due to time constraints of recontouring etc) this approach does exactly that - it focuses on the structures immediately adjacent to the tumor. Not a bad approach to consider in your clinic more broadly.
100% Rectal Ulcers
Next is a quick tale about some of his patients having rectal bleeding after high dose prostate cancer treatment. One of his brothers was a colorectal surgeon and to his “shock and horror every patient we treated, even though they were not complaining of anything, had an ulcer on the anterior rectal wall. Every patient. So the ulcer rate was 100% … that’s a bad thing right? You’re not supposed to cause ulcers.”
The moral of the story is that most of injuries that we cause will heal. Just like with the surgery analogy above, most heal. If you give high enough doses, you will injure the rectum. In fractionated treatment the most common reason for failure is radio-resistance but in ablative treatment many more are simply marginal misses “because you didn’t fully treat the tumor”.
Which leads to really bad outcomes by under treatment of the target - the cancer returns right next to structure that you limited dose due to the first time. Hence his priority of dose to target. Again I think it is wise to not be cavalier in your approach, but I think the point is not to under recognize the risk of recurrence.
They are useful only in relation to technology and approaches as exist today. With the future development of technologies and methods capable of creating, for example, ultrathin pencil beams, I predict we will be able to at least double the maximum dose tolerated by the spinal cord. Doing so would allow opportunity to eradicate tumors that today are rarely controlled. But it won't happen if we constrain such innovation, putting handcuffs on investigators who would otherwise explore better treatments. That's the danger of treating constraints like a religion derived from our current training and experience.
Where we go next: CUT
“My opinion is very different about how those constraints are used that’s made me rethink now how I should be talking to people about normal tissue constraints. Because if we don’t change how we approach these things how are we going to improve these therapies. How are we going to take SAbR to the next level.”
Can we accept injuries and simply allow them to heal similar to a surgery?
CUT: This is his anacronym for what surgeons do - they create a “Calculated Useful Trauma”.
We need to approach our patients in a similar way with the caveat that this “CUT” must heal. Again most of the emphasis returned not to contraints but to the prioritized principle of very steep dose gradiants as your primary path to achieve this result:
“Dosimetry needs to focus mostly on the gradients.… Our margins are where most of the toxicity from ablative dose occurs. So 0 margin treatment should be our goal. We’re not there for everything yet, but we’re getting there.”
For the high doses, use planning to remove hot spots from the nearby OARs and for the intermediate dose level, similar to a surgeon, you have to think about how this tissue will heal. If I damage these cells with radiation causing damage, how far will the “replacements” have to travel to rescue the tissue that I just damaged.
Surgeons reapproximate continuity so we need to think in a similar fashion - glancing blows rather than circumferential treatment.
He had a slide at the talk that I missed getting an image of - I’ve tried to re-create the concept below (technically this example has gel so don’t be too critical on the rectal contour). It showed this exact principle within the context of the rectal ulcer discussion. Basically he linked the non-healing ulcers to ones where a longer distance of rectum was treated due to shoe-horning of dose posteriorly. Here is my crude recreation of the two dose clouds simply with a contour. I think it is a very important message.

If you consider the green and red as two 95% isodose clouds (ie 2 plan options), the red has far more impact on the rectum. The cells to heal the ulcer will have to migrate further than if your isodose cloud looks more like the green. And yes, that difference MIGHT be visibly different on your DVH or in your checklist, but at the same, each might pass - but one is safer.
Below are notes from Dr. Ryckman that reiterates this theme:
Serial structures heal better when nearby stem cells can readily move to the injured area, implying that high dose circumferential radiotherapy of serial organs like the esophagus, rectum, or spinal cord should be avoided. Craniocaudal or nonadjacent stem cells can migrate to repair damage, so there is certainly value in nonadjacent wall sparing of luminal structures (so long as we are confident in our target volumes, of course).
Again, if you just listen to what he does - it makes sense. Cover the target and look really closely at the structures right next to the target and have a really steep dose gradient. He explains that he believes most of the toxicity we see is in the extra margin we treat around the cancer. All summed up in one picture that is easy to remember.
A Note on Serial vs Parallel Structures and Intermediate Dose:
From his tables paper:
The tables appropriately separate serial structures (tubes and wires) from parallel structures (organ parenchyma) as shown. This distinction is relevant because these tissues have very different strategies for avoiding dysfunction: Serial structures repair aggressively, and parallel structures take advantage of typically huge redundancy and reserve. Although the serial constraints are straightforward (effectively, “don't cross this line”), the parallel constraints follow the critical volume formalism and are best explained by Schefter et al. and Ritter et al. Rightly so, no mean dose limits appear in the tables. For highly conformal, gross-tumor-only treatments often just barely contacting adjacent structures, mean dose limits are easily shown to be meaningless for affecting toxicity.
And then from notes, we have a bit more detail where it is highlighted to think not just about where the dose goes, but where it doesn’t. I think more related to low and intermediate dose clouds. The example below is SBRT in lung - it is as important to have a volume of lung that is avoided. Here is a DVH from a paper Dr. Timmerman authored illustrating that point (Ref 5).
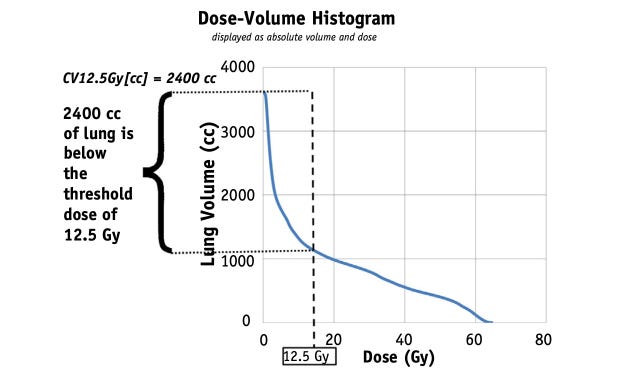
A common analogy today where this is a primary plan metric would be the treatment of liver cancer where we really prioritize the volume of liver spared.
And then finally a good discussion of the development and and then current use of R50 and D2cm. I think these notes add context to the discussion and again point to the simplicity of the initial approach. Cover the tumor and create a steep dose gradient and be really precise around nearby critical structures.
Notes from Jeff from his conversation:
R50 and D2cm have an interesting origin. A colleague was keen on using APPA SBRT for liver treatments. Despite the anticipated rib fractures, he believed it was the optimal strategy due to lateral intermediate/high dose spill. Dr. Timmerman expressed concerns about adopting the same method in the thorax, where AP/PA SBRT could lead to unnecessary rib fracturs, which would be avoided with a tighter dose cloud. Hence, R50 and D2cm were introduced to avoid AP/PA SBRT by "forcing" trialists to use more conformal techniques. Rather interesting, right?!
I won't use either metric in my clinic (unless on protocol). I do 2 cm shells but sometimes pull in 0.5-1.0 cm if close to a critical OAR, then ask for 50% IDL in the shell. It works beautifully. Please note, it gets more challenging to fit in tight shells with increasing lesion size, so more of the 50% IDL will “spill” out for larger lesions.
These metrics are essentially obsolete in the era of VMAT. The intermediate dose is important, and VMAT effectively replaces a good chunk of the intermediate dose volume with low dose volume. A recent report suggests only one out of three major facilities polled utilized R50 and CI for lung SABR cases.
Also Timmerman has metrics for conventional fractionation! I've compiled a table comparing Timmerman's conventional metrics to QUANTEC. I observed that Timmerman prefers absolute volume measurements (ccs) over relative (%), and I inquired about his choice.
Dr. Timmerman told me he had his physicist translate the percent volumes to absolute volumes. He uses absolute volumes in CCs instead of percent volumes to cut back on people who would cheat by making organs bigger to meet the percent volume constraints.
From my perspective, I remember shifting towards SBRT back well before VMAT and trying to hit the metrics using co-planar arcs and I could hit everything but these intermediate dose metrics. These metrics are what forced you to be non-coplanar in your approach so they absolutely worked back in the day in forcing a change in approach.
And then the notes are consistent with what you see in the marketplace today. Many programs have shifted many cases back to coplanar approaches - I think especially with less dose intensive schedules within VMAT programs - simply the number of beams and better modulation of leaves allows you to achieve better intermediate dose control than 5 or 7 coplanar beams.
Why Consolidate this Perspective?
First, it is incredibly valuable insight and secondly, I’m certain the masses misuse these tables. Most see them as litigation avoidance tools. I think our specialty needs a clear set of documents that show these, per the creator of the tables, were designed as rough guidelines - to point us towards safer approach but not intending to mandate hard stops.
In my experience, clinicians often want to push beyond these boundaries and I really believe the system is erring on the side of caution. So if it helps in a case or two, we have succeeded. Heck I had a rectal ulcer the other day that seems to now be healing, but for a moment, I was quite worried. The context of “it happened in every case” would have helped me to sleep better.
And then consider this story - the tables might not have EVER been published if he hadn’t stepped outside the traditional lanes.
Here comes a bit of devious brilliance. Joel Tepper asked me to be the guest editor of a Seminars in Radiation Oncology issue on the topic of hypofractionation. I did as asked and assembled a group of thought leaders who provided excellent contributions on the topic. For each Seminars issue, the guest editor is expected to write an introduction, which is actually referenced in Index Medicus. I decided to sneak the tables into that introduction, knowing they could never be published any other way. An extended table of constraints found in the article was titled “Mostly Unvalidated Normal Tissue Constraints for SBRT.” Now published and referenced, I have easily republished updates of the constraint tables many times by referencing the Seminars' introduction. Who says cheaters never win?
That in and of itself, makes the argument for more options in the distribution of information - like this Substack or the podcast - beyond the walls of the old structure.
In Closing:
In retrospect, the slide makes more sense. If I had been on this singular path for 25 years, I’d probably write something similar. And if this post gets another few people more comfortable in taking steps in that direction, then it was more than a worthwhile endeavor. I know I learned quite a bit, hopefully others did too.
Here, we like stories. Stories help give greater context. That is one of the goals.
Referring to the Red Journal Article, he said, “She said she’s going to do more of those, ask people who have stories to tell to tell stories which I think makes it funner.”
I agree and if stories makes this “funner”, so be it.
As always, thanks for following along with the journey as we search for better.
Special thanks Jeff Ryckman for the notes and helping making sure all the context was correct. A shout out to Simul Parikh and Matt Spraker and Nina Sanford for the podcast episode which was great and yep, Bob Timmerman who did give this a final ok.
ADDITIONAL REFERENCES:
Stereotactic High Dose Fraction Radiation Therapy of Extracranial Tumors Using an Accelerator:
https://www.tandfonline.com/doi/pdf/10.3109/02841869509127197Stereotactic radiotherapy of malignancies in the abdomen. Methodological aspects
https://pubmed.ncbi.nlm.nih.gov/7946448/Indiana Phase II study - lung cancer:
https://pubmed.ncbi.nlm.nih.gov/19251380/RTOG 0236:
https://pubmed.ncbi.nlm.nih.gov/29852036/Application of Critical Volume-Dose Constraints for Stereotactic Body Radiation Therapy in NRG Radiation Therapy Trials
https://pubmed.ncbi.nlm.nih.gov/28587050/