


Protons 101: The Opportunity for Protons to Improve Outcomes in Breast Cancer
A deeper dive into the rationale and expectations for the ongoing RADCOMP and PARABLE Trials

As always, author of one. If you see an error or omission, please contact me or comment and I’ll work to address it.
RADCOMP and PARABLE Trials will help define the role for proton therapy in the treatment of advanced breast cancer.
The rationale is quite simple. Radiation dose to the heart is related to long-term risk of major cardiac events. Proton plans can significantly reduce heart dose for some breast cancer patients (estimated to be about 1-2 in 30 left sided cases).
First things first - tangent breast cancer treatment is an excellent treatment with very little toxicity and clear overall survival benefit. When paired with things like surface guidance and or breath hold approaches, tangent treatment is the treatment of choice for the vast majority of even left sided breast cancer patients. In fact, as you see above, best estimates are that 28 or 29 out of 30 patients will be BEST served with traditional tangent treatment. So when you see a Tweet like the one below from a large cancer center or something similar on a breast cancer proton webpage, just remember it should have much more context. (This is sad, but it a reality today broadly across healthcare marketing).

TAKE HOME MESSAGE FOR PATIENTS - If radiation is required for treatment of your breast cancer and your heart mean dose is >1Gy or the LAD dose is greater than v15>10%. Ask about breath hold. Ask why the numbers are so high? Consider a second opinion at a proton center so you can see a comparative proton plan for your cancer (I consistently meet both of these on nearly every plan). Tangents are generally very good breast cancer treatments and these metrics should be able to be met. IMRT is generally not nearly as strong specifically for breast cancer but if it meets the above requirements, you have a safe plan for your heart.
IT IS THE EXCEPTIONS THAT MAKE THE CASE FOR PROTONS: Primarily when Comprehensive Lymph Node Treatment is required specifically to the IMC lymph nodes.
And this is the focus of the RADCOMP Trial specifically (ref 1). The PARABLE trial (ref 2) is more nuanced requiring two plans - one non-proton plan and a proton plan. Patients are then eligible IF there is a significant dosimetry difference that predicts higher cardiac toxicity. But they each strive to study proton therapy in a group at higher risk of cardiac toxicity due to radiation to the heart and lungs.
Below is an example of one of these exception cases where protons have great potential. The left is IMRT, on the right is a Passive scatter plan - a more advanced PBS plan would be one small step better. We are treating the lymph nodes in the IMC (internal mammary chain) region because it is a more advanced cancer than most. As you can see, heart and heart substructure dosing is far better with the PBT plan. There is NO risk of breast cancer spreading to the heart. There is NO reason to deliver any dose to the heart.

Example 2: A more advanced case - young patient, we needed to aggressively cover the left chest wall in a comprehensive fashion and we should keep heart and lung radiation dose to a minimum.

These are the types of examples that make me laugh when some radiation oncologists make crazy arguments on social media sites that protons have no role in breast cancer. They have a role, we just need it more precisely defined.
In recent years (my opinion), proton beam has been vastly under utilized for breast cancer with a national utilization rate of 0.2%. If 1 in 60 (from the PARABLE TRIAL, ref 3) is correct, then this number should be 1.667%. That would be a minimum of 3800 women each year in the US not treated with proton therapy according to the PARABLE risk stratification analysis.
And note, IMRT is utilized 6.9% so that would be closer to 15,000 patients (rounding down significantly due to some APBI) that potentially get significantly better treatment with protons. (I really like IMRT, but for breast cancer, it simply is not ideal in my clinical assessment).
These are not inconsequential numbers of patients that can be impacted.

The Opportunity primarily relates to decreased Cardiac Toxicity.
Cardiac Toxicity from Breast Cancer radiation has been an area of interest for me going back decades and we have come a long way!
Special shout-out to Dr. Tom Buchholz. This study that I worked on was certainly not my idea as a resident at MD Anderson, it was his. He was one of the three leads on the breast service back in the day with Marsha McNeese and Eric Strom and together we published the small study below (ref 4). It is one the first papers published looking at radiation doses delivered to the various blood vessels of the heart. There are a few maybe earlier looks, but not many.

In this study looking at dose to the LAD from 2001, a 5mm change in perpendicular lung distance represented a 20% difference in the volume of LAD treated to 20Gy. Today our most verified cardiac substructure metric is the LAD where the volume treated to 15Gy should be less than 10%. So yes, we are making progress and pushing doses far lower than even just 2 decades ago with greater awareness of the issue and tools like breath hold. In other words, radiation oncology believes in the principle that radiating the heart is bad and that excess dose should be aggressively minimized.
Mean Heart Dose - The first proven metric
The New England Journal Darby paper in 2013 pushed our field further.
It showed a linear relationship between mean heart dose and major coronary events - higher radiation dose, more heart disease. Following its release, there was an increased focus on reducing heart dose.

This was a landmark paper. It shows a few important things.
THERE IS NO SAFE LOWER THRESHOLD - GOING ALL THE WAY DOWN TO DOSES BELOW 2 GY SHOWED AN INCREASE IN THE RATE OF MAJOR CORONARY EVENTS.
THE IMPACT OCCURRED A ALL AGES AND RADIATION INCREASED YOUR RISK WHETHER OR NOT YOU HAD EXISTING RISK FACTORS.
EVERY GRAY (UNIT OF RADIATION DOSE) RESULTS IN AN INCREASE OF 7.4% OF YOUR OF SUFFERING A MAJOR CORONARY EVENT.
Today, I think this data continue to be refined somewhat, but the principles of this first critical trial hold true today.
How do heart and lung doses compare for PBT vs. IMRT?
Here are two studies published in 2018 (ref 6,7) - both out of Memorial Sloan Kettering - a true top tier institution in our fight against cancer. In the first study, they report outcomes for breast cancer treated with IMRT from 2010-2013. IMRT methods have evolved and doses can be lower in some programs today, but in many US facilities, I don’t think this is unreasonable data to illustrate a meaningful difference. In the second study, they report their outcomes for breast cancer treated with passive scatter proton therapy.
MEAN HEART DOSE: ~11 GY FOR IMRT, 0.7 GY FOR PROTON THERAPY. IMRT GAVE 15 TIMES THE RADIATION TO THE HEART.
IPSILATERAL LUNG: BASICALLY ALL THE LUNG ON THE SIDE OF THE TUMOR RECEIVES 5GY OF RADIATION WITH IMRT, WITH PROTON THERAPY ABOUT 34% RECIEVES 5 GY.
The argument against this data is often as simple as:
“Sure but I don’t treat that much heart. 11Gy is ridiculous.”
And for some programs, that might be as doses are moving lower with improved tools like VMAT and breath hold techniques. But you can’t get to proton doses or the dosimetry pictured at the top of this article. But to appease, cut it in half - 5.5 Gy or even to 1/3rd to 3.66 Gy mean heart dose. Compared to 0.7 Gy, those doses remain a large scale difference if the Darby data is close to correct.
LAD Dose - My second cardiac breast cancer dose metric
The LAD runs right along the front of the heart - closest to the breast - here is a picture - this one has a lot of calcium in it (pt likely has risk factors like older, high cholesterol, high blood pressure etc) but it shows you where the vessel tracks - from here it runs along the front left (picture right) side of the heart - basically the closest part of the heart to the radiation target and its dose can be dramatically affected with relatively small changes in the plan making it critical to assess.
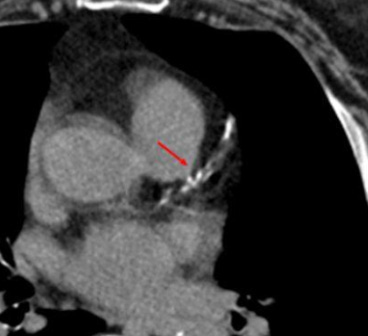
The best data is from lung and that is where I have taken the V15<10% metric - less than 10% of the LAD needs to receive 15 Gy. Remember from my old study that a 5mm difference in chest anatomy makes approximately a 20% difference in the volume of the LAD receiving 20 Gy when treating with tangents for breast cancer - so small differences in anatomy matter.
In the lung cancer trial RTOG 0617, if your LAD was treated above this metric of V15>10%, your two year survival was 47% (high LAD dose) vs. 67% (low LAD dose) (p=0.004)(ref 8). Its an advanced lung cancer trial so survival is quite poor at 20.2 (high LAD dose) vs. 25.1 months (lower LAD dose) - but the concept is simple. Radiation appeared to clearly cause heart disease. And not years down the road - early major cardiac events that affected 2 yr survival. And the data appears to hold up in breast in a study from Beaumont Hospital in Michigan with higher LAD radiation dose having more cardiac events (ref 9).
In summary, there are decades of data that I only briefly touched upon that clearly show radiation damages the heart. Excess radiation to the heart simply results in excess cardiac deaths.
Proton therapy has proven benefits in reducing heart dose for breast cancer when tumors are more advanced and nodal irradiation is required. Even with this information, proton therapy simply isn’t used outside of rare instances.
This IS the opportunity. But as I’ve said before, proving that a dosimetry difference results in improvements in outcomes is difficult work.
So that is simply stated the goal of the RADCOMP and PARABLE trials - take patients at significantly higher than average risk of developing cardiac toxicity directly due to radiation to the heart and see if that group truly benefits in PBT is substituted for traditional treatment. While it is easy to presume to know the answer, changing treatment outcomes is far less likely than is often thought. The answer is to do trials like this - in a prospective randomized fashion and determine the answer via science.
If the trial is negative
The retrospective data is strong. The entire medical specialty of CardOnc (cardiac oncology) has been created as we acknowledge that treatment results in damage. If negative, we’ll need to parse for passive scanning vs pencil beam and left sided vs. right sided disease. We’ll need to further evaluate cardiac substructures dosing. Simply stated, we’ll have work to do.
And if negative, I’ll look to the RADCOMP Ancillary Study (ref 10) that prospectively studies 155 patients with far more detailed cardiac measurements to help glean more information. Primary metrics in that study include: Left ventricular fraction, Right Ventricular Fractional Area Change, N-terminal pro B-type natriuretic peptide, Placental Growth Factor and Growth Differentiation Factor-15.
If both are broadly negative and dosimetry metrics persist, we will have missed something and it will be a blow to the industry.
If the trial is positive
It will be a matter of watching to see how the market reacts and adjusts to the data. This is a significant percentage of breast cancer patients and in my view, there is NO WAY, these patients will be routinely referred out of non-proton therapy institutions to institutions with the technology overnight. Our US healthcare system simply isn’t built that way.
And if Protons are Better, Next up: APBI
If the above trials are negative (where the dosimetry differences are greater), this argument to me becomes moot. But…if it is positive, I’ll leave with the next area that can be evaluated - again, simple tangents isn’t an area where there are any expectations for improvement, but in APBI - partial breast irradiation, lung and heart doses are often held to near zero with PBT. This is not the case for IMRT approaches for partial breast treatments.
 vs a heart optimized IMRT plan (below) Mark Storey MD")

I think that is the opportunity for protons in breast cancer. With over 1200 patients in the study and lots of patients treated with pencil beam in a patient population where we believe we have good metrics, this should be a win. But as I’ve said, it is very easy to over estimate medical technology improvements and often, the true path and the true science is much more nuanced. Time will tell. The trial is scheduled to close to accrual in 2023 or early 2024.
REFRENCES:
Breast Cancer RADCOMP Trial:
https://clinicaltrials.gov/ct2/show/NCT02603341PARABLE Trial:
https://www.icr.ac.uk/our-research/centres-and-collaborations/centres-at-the-icr/clinical-trials-and-statistics-unit/our-research/clinical-trials/parablePARABLE Commentary for the ratio expected to be eligible.
https://www.nihr.ac.uk/news/first-uk-proton-beam-therapy-trial-for-breast-cancer-launches/32346Coronary artery dosimetry in intact left breast irradiation
https://pubmed.ncbi.nlm.nih.gov/11769861/Left Anterior Descending Coronary Artery Radiation Dose Association With All-Cause Mortality in NRG Oncology Trial RTOG 0617
https://www.redjournal.org/article/S0360-3016(22)03565-9/fulltextLong-Term Pulmonary Outcomes of a Feasibility Study of Inverse-Planned, Multibeam Intensity Modulated Radiation Therapy in Node-Positive Breast Cancer Patients Receiving Regional Nodal Irradiation
https://pubmed.ncbi.nlm.nih.gov/30508620/Early outcomes of breast cancer patients treated with post-mastectomy uniform scanning proton therapy
https://pubmed.ncbi.nlm.nih.gov/30414757/Left Anterior Descending Coronary Artery Radiation Dose Association With All-Cause Mortality in NRG Oncology Trial RTOG 0617
https://www.redjournal.org/article/S0360-3016(22)03565-9/fulltextDose to the Left Anterior Descending Artery Correlates With Cardiac Events After Irradiation for Breast Cancer
https://pubmed.ncbi.nlm.nih.gov/35483540/Cardiotoxicity in Breast Cancer Patients Treated With Proton or Photon Radiotherapy: A RadComp Ancillary Study
https://clinicaltrials.gov/ct2/show/NCT04361240www.protons101.com, home of the original Protons 101 website.
Content for the Protons101 blog written by Mark Storey MD.