
How do we compete within a framework of massive financial imbalances?
ASCO made me think - how can radiation oncology move forward along a better path for its future.

If you believe that billions of dollars do not impact outcomes - Ask the PGA tour. Ask our US government who, as the economy turned south looked to Saudi Arabia amongst others to increase oil production. Idealistic positions in the face of massive dollars too often today do not hold up under the weight of these imbalances.
But I think we can do simple productive things that help shift our field to a stronger, more unified approach. Today, we’ll give some context to the degree of imbalance and look at just one example where I think we can make improvements to our fields approach.
The Scope of the Financial Difference:
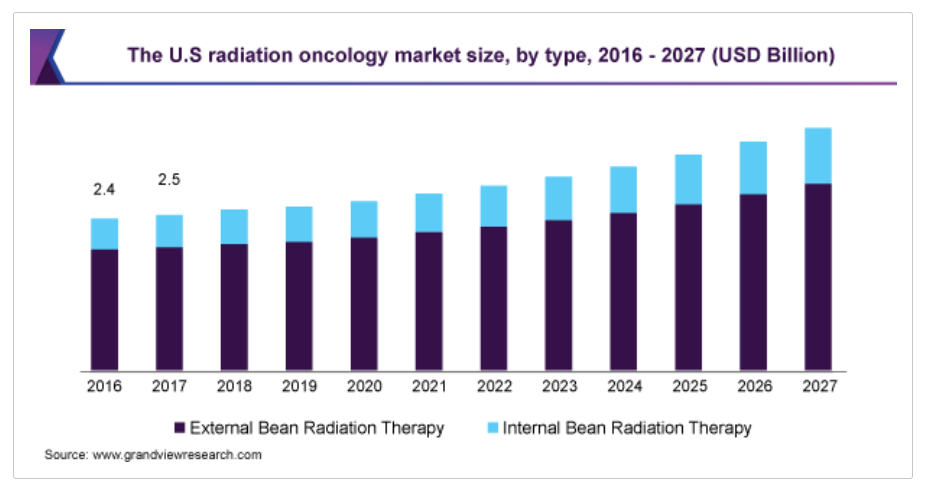
A few starter facts: references that show the scale of the issue. First radiation oncology - a 3B US market size entity (ref 1).
Compare those numbers to the leading 10 prescription drugs based on US sales. Note: Our entire field would not be listed below - these are single drugs - US market revenue only (ref 2).

And Pfizer - the broader company:
Revenue in 2023 (TTM): $92.95 B
According to Pfizer's latest financial reports the company's current revenue (TTM) is $92.95 B. In 2022 the company made a revenue of $100.33 B an increase over the years 2021 revenue that were of $81.49 B.
Pfizer alone is 30x the size and scope of our field in the US.
And the broader pharmaceutical industry? A 1 trillion dollar industry - half in the US.
How much is the pharmaceutical industry worth in US?
United States: According to an article published by Zippia, the US pharmaceutical industry generated $550 billion in revenue in 2021, accounting for 48% of the global pharmaceutical market as of 2020.Feb 7, 2023
Comparing Global Pharmaceutical Markets: US, UK, and China, pharmanewsintel.com
Obviously the $1T is all medications but many of the high fliers cruise in our airspace waaay waaay above the basements where linear accelerators live.
As I said, there is imbalance:
And now just for a moment consider how pharma approaches the oncology market. Let’s look at number 2 on the list as an example, because it is directly in our space.
Keytruda - a wonderful drug, but $9.8B - likely 3x our entire field and while it is a good medicine - Keytruda or radiation (plus 6B per year in technology upgrades for our field)?
Radiation is far more valuable. And I really don’t think it is close for the value the two provide to oncology. (if you disagree please comment)
But as a mental exercise just think about any ad for any drug.
Pretty people, perhaps sad at the start but once the drug kicks in, all are happy and living in beautiful environments. And during that last part - where the images are so very positive, they run that sped up voice covering of the toxicities for the drugs - can cause an increased risk death, suicide etc. etc.
They include these risks, not because they want to or because they have high morals. It is a legal requirement but very purposefully, they make it as small of a segment of the ad as they legally can and the voice is probably sped up to the maximum legal limit and they try to wash it with the imagery. This is all purposeful to sell their drug and absolutely minimize discussion of risks. And the marketing budget for that SINGLE drug is bit under $100M.
Next consider radiation:
Where from my seat (again notably slanted), protons are considered “big spending” - and yet the entirety of the proton therapy industry is literally a rounding error on the US pharma marketing budget.
And so to me, it is not surprising that multiple articles with rather negative slants have appeared over the last year or two with respect to radiation oncology. Radiation immediately brings forward thoughts of nuclear disasters and atomic bombs - Chernobyl, Hiroshima. Really, really terrible things. And everyone knows to avoid it. Think about the difficulty and pushback implementing x-ray screening at the airport. And then think about just how fractured we are as a specialty - even as a very small field within medicine. There is likely some faction of our own field that won’t read this site due to the word “proton”. So to me, negative headlines are not surprising.
And then, as if to make it worse, look at our own - “advertising." This is essentially one of our largest “campaigns” since I left training. It pairs nicely with our work to shorten treatments and de-escalate our own use. It reminds us, and others, the ways in which we are “wasteful” (ironically at a fraction of the cost of some drugs that may or may not benefit recipients).
ASTRO Choosing Wisely.
I’ll summarize:
Don’t, don’t, don’t. And if you really have to radiate someone, please, please do as little as possible.


It reminds me of an ACR question I was given for ongoing certification about 2 years ago - the answer they WANTED for the most common reason for a major side effect was LITERALLY GROSS NEGLIGENCE by the radiation oncologist. Specifically it was treating the whole circumference of the leg causing terrible lymphedema when it was not required or justified by the cancer. Was it the cancer extent or surgical approach or a combination of issues? Nope - it was BAD radiation given by an ignorant doctor - that was the most likely reason / “best” answer. There they are - our professional society and our accreditation board “promoting” our field.
Pair that with an inherent basic fear of radiation in the public and it should be no surprise why the New York Times inserts “brutal” next to radiation.
Meanwhile 9 weeks vs. a year of Herceptin maybe improved survival by a percent and it is a pretty clear answer - yep, need a year.
Local vs. National Approach
So while I agree with some that really encourage us to be active on a local or regional level as physician leaders in our community, I’d ask: is that enough?
I believe we need national leadership with a more unifying message. Really, I don’t think that should be questioned. One last example:
A good friend of mine started a program for intentional tremor - in private practice. Somehow there was communication from a national university where an attending started chastising the guy in practice that absolutely he was wrong and that it was reckless and dangerous.
Here’s the funny part: The equipment was newer in the private setting - generations newer than at the university. The MD in private practice had decades more experience (both in volume and years) than the far younger academic physician regarding high dose SBRT in the brain. And when pressed - the academic radiation oncologist was NOT really involved on any level with the contouring, struggling to answer some of the more nuance anatomy / imaging / MRI sequencing questions - turns out all contouring was done outside the radiation oncology department via neurosurgery and radiology. Whereas in my friends practice - he drew the volume sitting alongside those same experts from the other fields.
But is/was there a national statement where we recommend this type of broadening of our impact. No. In fact, the tone of ASTRO today and the tone during the physician’s training was - at least on some level - some people are doing really, really bad stuff - stuff that is harmful to our specialty. And I think it carries over in a lot of subtle ways. And that is my point, there will always be some disagreements and differences in opinion between physicians but here - I really do believe that a more unified national voice might have led to a far more productive discussion. Here I think the divisive tone impacted the interaction. In contrast, we should be working together to help build the programs rather than an us/them reaction.
For intentional tremor, 19 year data was published in 2017 (ref 3). Personally, would I do it? - don’t think so - I’d need a half decade or more of more focused work in that region to feel comfortable. But to me, whether that is expanding indications to benign disease or debating benefits of capital technology spend - we need to find ways to be supportive and present a more unified voice - at least beyond the locker room discussion within our specialty.
In medical oncology, they can debate and bicker all day long because, at the end of the day, there are ads for Keytruda or Opdivo as you watch TV in the evening or search online. The positives ABSOLUTELY win out and overwhelm any disagreement between treating physicians - marketing dollars, and lots of them, are impactful. Our specialty is fundamentally different. I’ve NEVER seen a Varian or Elekta add discussing rectal cancer - saying - remember talk to your doctor about the benefits of radiation to help avoid ostomy and reduce chemotherapy related neuropathy. In our field, we are the lone voice.
Consider IF we were much closer to 100% united - a $3B industry completely united - focused on promoting our value and looking for ways to enhance our use and extend our reach. I think this is our hope.
Why do I think we might compete at $3B when still out funded by tens of billions of dollars?
Because we offer tremendous value in healthcare and voices are beginning to come around that demonstrate common sense. Enough is finally approaching enough.
I appreciate it is quite ironic that this discussion is on a proton named site. Protons are a poor example of value when compared to the rest of radiation oncology but on a broader look, other options - like for example years of 100k+ drugs for secondary endpoints that likely don’t impact real patient outcomes have simply blown by the increased costs of protons. That doesn’t make the lack of data excusable, but what once appeared to be a stupid level of expense is now dwarfed by stupider pharma expense. And it is backed by massive marketing campaigns and huge investments into the scientists that run the trials - and those campaigns purposefully seek to capture and maximize potential revenue streams.
And finally on the proton side, we have good trials running with better technology using pencil beam approaches. And as I’ve said, if they are negative, I’ll move protons into this discussion.
So to complete today’s exercise, let’s consider rebuilding the Choosing Wisely list: Just an idea.
CHOOSING WISELY: CHOOSE RADIATION
Radiation offers tremendous value in early breast cancer but it is being omitted or substituted in favor of years of estrogen blockers. Enroll patients in our national trial comparing radiation to 5 yrs of hormonal therapy for eligible women.
Engage surgeons and medical oncology to discuss the advantages of dose escalation approaches in some rectal cancers where a combination of chemotherapy and radiation is proven to allow more patients to avoid a long-term ostomy. And similar to lymphoma, have discussions regarding the role for radiation to substitute and often lower total patient toxicity through a combination of modalities rather than simply increasing the duration and intensity of chemotherapy.
Hypofractionated or SBRT high dose approaches are proven safe and effective in most prostate cancers where often we can limit or eliminate ADT. Radiation provides less toxicity than surgery and has proven superior cure rates than Hifu, Cryo or Tulsa approaches with decades of long-term proven outcomes.
Be adamant in tumor boards and with other specialist regarding the role of radiation in the treatment of liver disease from cancer. Data continues to accrue demonstrating our superiority to other approaches. Our technology driven approaches allow for high doses today to these tumor that was not possible just two decades ago.
Radiation is a wonderfully cost effective benefit to patients with metastatic cancer - in fact, many with limited disease - called oligometastatic disease, can be potentially cured. And those with more advanced disease can see great long-term control with localized approaches to target painful regions - often in just a few sessions.
Important trials attempting to demonstrate benefit with proton therapy are ongoing today. Nationwide we are enrolling patients in important trials in lung, esophageal, head and neck, and locally advanced breast cancers just to highlight a few. Support these efforts to help define which patients might benefit from this approach.
ASTRO is partnering with pharmaceutical companies to run several immunotherapy trials across a variety of disease sites where there is promising data supporting dual treatment approaches. Support these trials and encourage enrollment so we can quickly define those that benefit from this novel approach.
Remember that benign disease is often overlooked as a place where there is clear long term benefit for radiation demonstrating value and quality of life improvements for those patients. Radiation courses for these diseases are often only a few sessions and might enable patients long-term relief while limiting or eliminating the need for medications.
Promote our field beyond our traditional areas of expertise. We have exciting progress beyond cancer in the field of cardiology and neurology where we can assist with altered heart rhythms or tremors using targeted and highly precise delivery of radiation to small portions of the heart or brain where nerves are malfunctioning. Consider methods to integrate these newer approaches into your practice and expand our reach.
Support ASTRO’s new educational programs that look to better integrate immunotherapy and concurrent drug regimens into our training for future and current radiation oncologists. It is imperative that we embrace and partner with pharmaceutical companies to help best define where that partnership can create the greatest value.
Be advocates with your administration on a local level regarding the need for new capital equipment purchases. New purchases allow us to pursue improvements in limiting dose to ever shrinking targets and allows the treatment of less normal tissue. For some it might be cone beam or breath hold systems or surface imaging while for others it may make sense to consider MRI linacs or proton therapy investments.
Finally, help advertise our value. We provide care across a spectrum of diseases - often curative approaches at a fraction of the costs of other approaches. We are a small industry especially when compared to the broader pharmaceutical industry and we need all parties to support the value we bring to oncology on a daily basis. With your help, we are and will continue to be an integral part of oncology as we move into the next century.
(1 person - 15 min exercise - certainly could be improved)
Now read the two back to back, and then, ask yourself which better represents our field as we move forward.
To me, at least, I think the answer is pretty clear. As individuals we must continue to do great work within our community, but the tone at a national level must change. As an specialty, we need to be united - focused on the value we provide. I strongly believe in that value and believe there is great opportunity to push our field and the care we provide for our patients forward as we demonstrate leadership within the field of oncology.
REFERENCES:
https://www.grandviewresearch.com/industry-analysis/us-radiation-oncology-market#:~:text=The%20U.S.%20radiation%20oncology%20market,the%20growing%20adoption%20of%20radiotherapy.
https://www.statista.com/statistics/258010/top-branded-drugs-based-on-retail-sales-in-the-us/
Stereotactic radiosurgery for essential tremor: Retrospective analysis of a 19-year experience
https://pubmed.ncbi.nlm.nih.gov/28319282/
I completely agree