


A Physician Perspective: My COVID journey and how it will forever alter my interpretation of medical literature.
I always new that science and money and power intersected in the medical literature, I just thought that, in the end, science won.

The following is my story through COVID. These are my personal events and my experience. It touches upon how that now translates in my reading of the oncology literature at large and will impact my practice of medicine moving forward.
About me:
I’m a radiation oncologist. I graduated medical school in 1996, completing training in 2001. I was blessed to have the opportunity to perform my residency work at MD Anderson after getting a undergraduate degree in engineering at Vanderbilt and medical degree at Arkansas. I joined an 8 person practice in my home state of Arkansas and practiced in North Little Rock for about 17 yrs. In that period I served as President of our group for about 10 yrs. We contracted with a non-profit and in its history our practice built up nearly 100M (around 75M during my time) in assets in that non-profit entity. Those funds were utilized to create a multi-specialty organization with a large cancer facility. Around 2016, I started looking at proton therapy more seriously as a way to help my patients - particularly head and neck cancer patients reduce long-term toxicity from treatment. In 2018 an opportunity to come to OKC and help lead the restructured Oklahoma Proton Center as Medical Director was offered and in a mid-life crisis of sorts, my wife and I moved to OKC.
I have a solid background for reading the medical literature and I think I’ve always been quite an independent physician / thinker. In fact I joke that I’m fiercely independent - always a contractor or independent and never an employee of a hospital (since leaving residency). I’m currently a practice of one doing my own thing as I choose to do. As an undergraduate, I have nearly a math minor in mathematics with an engineering background. At MD Anderson we had dedicated stats courses and even a weekly off-site statistics boot camp in the NE that I had the privilege to attend. I’ve run my own statistics since back in the 1990’s. To be clear, I’m no statistician but I’m not ignorant to the math methods used in papers to make arguments. I pair that above average mathematical medical background with stronger business experience than some 98% of physicians (a guestimate) - leading the group in Arkansas at a board level as we did bond development, transition to a multi-specialty cancer program, contract restructuring, capital outlays etc. and then in OKC participating in purchasing the center via federal bankruptcy, stabilizing and growing the business, and then see us successfully restructure it via a SPAC into the current non-profit entity.
I point these things out to give context and background. This Substack is a new venture and while I’ve tried to add enough details to validate some of that relevant experience, I’ve also purposefully been a vague with naming institutions and individuals in some areas where those details serve little to no benefit at this point.
My COVID story:
I remember standing up to make an announcement that our cancer facility would stop having weekly buffet luncheons. It was a Wednesday back in March of 2020. Actually it would become “that Wednesday”, but let’s keep some focus.
I live in Oklahoma, a pretty conservative state. As I talked at the luncheon about the new virus and the fact that, as a cancer center, we just could not keep having group social gatherings where we ate off a buffet line, there was a clear impression that I was the crazy one. There weren’t outright boo’s but there was definitely some moaning and gnashing of teeth.
But as Medical Director of a large multi-room proton center, we needed to be cautious. There had been a single case reported in Tulsa just a week earlier. He had a clear travel history putting him at risk and people were “sure” at the time, you needed a direct exposure to Italy or China or a part of the world where this virus lived. It was very early in the pandemic but shutting down the luncheons seemed correct. I was on small weekly calls with leadership from US leading institutions across the country - from the University of Seattle to Memorial Sloan Kettering and about 10 other major hospital metropolitan centers in between the two. There was risk, and it was very real, and it would be on our doorstep soon. At this time in the pandemic I was clearly an outlier as one of the most cautious people both inside and, after the luncheon, outside the center in my small world on the north side of OKC. It was weird experience for me to be that far from mainstream opinion but as a physician leader of the center, I wanted us to miss being careful.
That night, I turned on the Oklahoma City Thunder basketball game to watch live as it was cancelled. And in an instant, the world had changed. NBA basketball and other major sports were cancelled and it clearly was now in Oklahoma City. The next day as I returned to work, there was clearly less irritation regarding my decision to shut down the lunches. It made more sense and maybe, just maybe, I wasn’t the crazy one. Maybe the pandemic was going to be bigger than a free center provided lunch buffet.
Internally at the center, we started working on policies in house trying to minimize risks. We masked early in the pandemic. We limited aerosolizing procedures. We delayed a few lower risk treatments where I really thought there was minimal risk - mainly prostate cancer patients receiving ADT. That said we stayed open and kept treating patients never moving to less than about 80% patient load. I always disagreed with the radiation oncology narrative of giving chemotherapy as a safer alternative - we are subspecialty whose greatest strength seems often to be weakening our own future - but that perhaps is a topic for another day.
As everyone knows, early on, it was a roller coaster. We were masking and taking temperatures and screening at entry, but the large hospitals in town moved at institution speeds for a conservative state. They were still not masking - even going so far as to not allow their oncology employees to wear masks due to the fact that they could / would scare their patients. It was during this early time period, while we were masking and the hospitals (at least some of whom) were actively disallowing their staff to mask, that a CT I had ordered came across my to do list. A simple chest CT.
I opened up the chest CT to review the images and it looked like a Twitter COVID case - at least the CTs of COVID that I had seen on Twitter. Maybe there was a publication or two, but really it was Twitter images that had me consider it. This was a cancer patient who appeared to have COVID with bilateral lung disease typical for this new disease. I called radiology and spoke with them asking about why COVID wasn’t considered - it wasn’t in the report or impression or even mentioned but appeared to be in the differential from my review. I called radiology and they agreed - Yep, likely COVID but they had been told to not call so many. At that moment high stats for the hospital were perceived as bad and they didn’t have a lot of excess isolation rooms so in the last week or so, administration had asked them to make less COVID diagnosis calls.
How far the pendulum would swing. Again, that was an oncology patient who, at the time of my call to radiology, had been to our clinic for a simulation earlier that day and was actively sitting in a room with other oncology patients receiving chemotherapy in a facility where staff were not allowed to mask even if the nursing / care team members wanted to. This was a time of chaos as the disease landed at our doorstep. And we did a poor job in making basic decisions.
I want to make this clear, I was far from perfect. I saw the global infection coming and pulled some money out of the stock market but missed the bottom and ultimately would have been better off to stay invested. I saw a tweet online (note: from the future White House Coronavirus Response Coordinator) I thought was overstating facts creating undue fear and, in hindsight, my only COVID tweet (that I recall) was wrong. Millions of Americans were soon infected. China’s lockdowns were far more severe and their data was likely very inaccurate and the extent of disease here in the US was likely very understated / under appreciated. There clearly were people closer to the inner circle than myself.
(I strongly recommend reading Alex Washburne’s journey, The Predictive Theory of COVID-19, Ref 1. For me, it helps explain how I was wrong just reading a surface exposed narrative. Yes I had some inside weekly calls, but it still was a narrative which I believe now others knew to be partial at best and it provides great insight into this initial period in our history.)
So I wasn’t perfect, but I have followed this closely for a long time (admittingly far less closely since the summer of 2022). As one simple example, here is illustration from my personal archive showing rapid deterioration of the University of Washington hospital modeling data (Ref 2) that was driving public response and public policy. In just 14 days modeling moved hospital bed utilization from 4763 to 882 for Oklahoma (Pictures were captured April 6th, 14th, and 20th 2020 respectively). The old model would “vanish” and be replaced with “new” “answers”. I should have known then that we were going to overshoot on response but I very much stepped in line and followed direction as we tried to “flatten the curve”.
April 6th Model: 4763 beds.

April 14th Model: 1391 beds
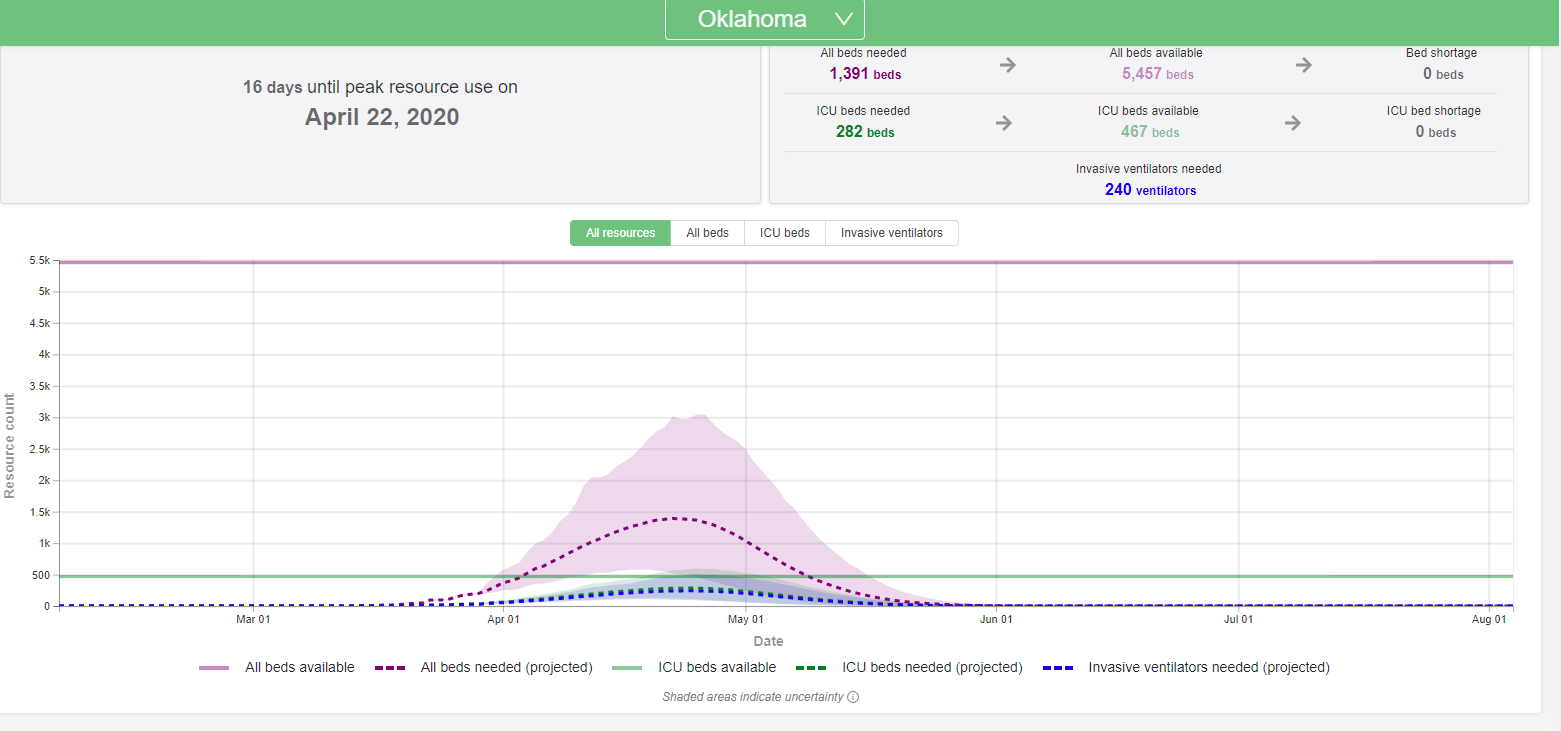
April 20th Model: 882 beds
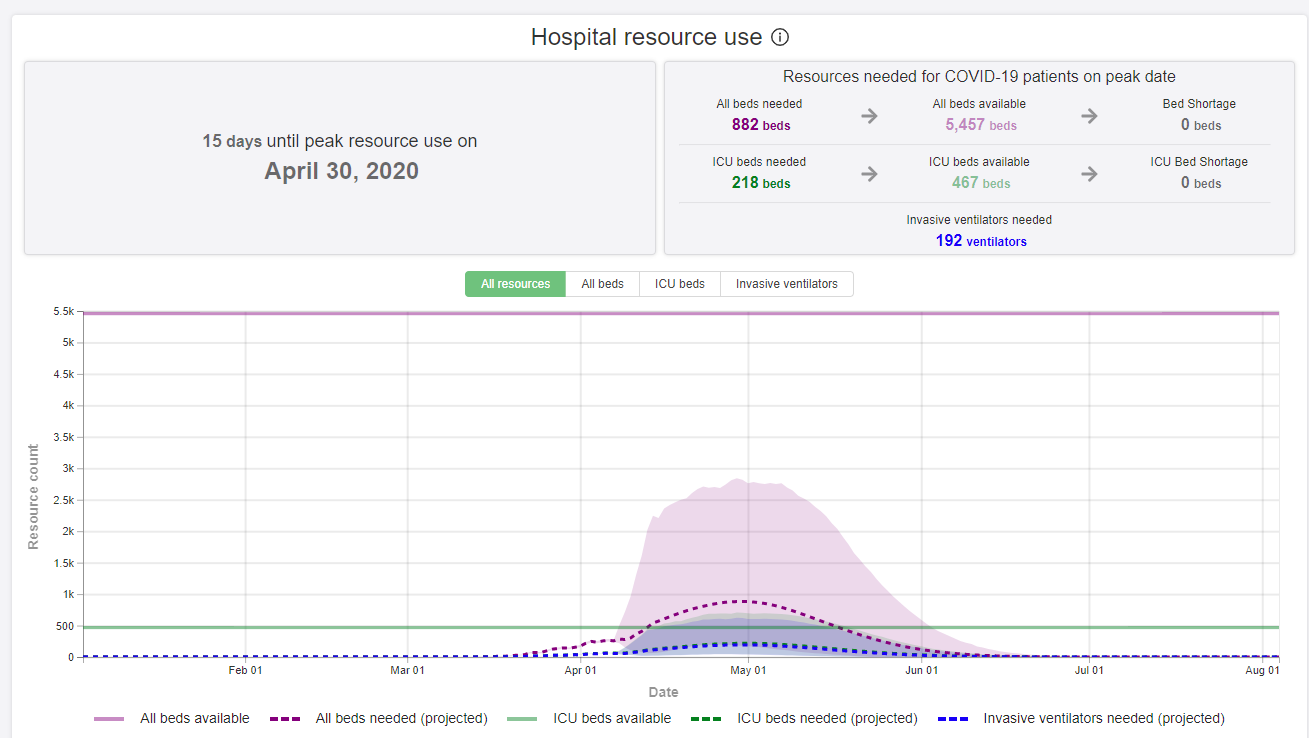
So with the benefit of hindsight, clearly the radiation oncologist wasn’t perfect, but neither were the expert modelers that we were basing our response upon (note in the reference, you can’t event get back to the times shown above).
Regardless, we move on. A new normal began. The Oklahoma Proton Center was a two MD facility and I pretty much shut down all travel beyond home and work. I tried to be very careful for both myself and my patients. In our weekly national meetings, I heard very significant tales from the two coasts and we worked hard to stay ahead of any issues in Oklahoma and within our facility. That was required as a provider of cancer care.
My daughter was at college during this time - her institution had large scale representation on some of the highest level national healthcare boards making decisions for our country regarding COVID policies. She was in and out of lockdown based on both real and questionable exposures. She could take Tylenol but was told not to exercise or take ibuprofen. In total she spent about 1 month in lockdown. We offered a trip home but she wanted to stay at school. We knew little regarding management of the disease so I commonly recommended the institutions medical advise to any of my patients as information regarding what to do if one was infected as they clearly had inside sources regarding how best to treat a new case - or so I thought at the time.
Around the time of the initial vaccine rollout in late January of 2021, my daughter tested positive for COVID - lost taste and smell and was pretty sick for about a week to 10 days. (She has recovered and is well now.) A few weeks post her recovery, the first vaccine was released and pretty quickly, her university mandated all students be vaccinated - regardless of prior infections. Based on the applied pressure, she wanted the vaccine and it was the only way for her to stay at school with any level of freedom so I stayed quiet and we moved forward but my antenna went up that things really were becoming more of a narrative and less about data.
In hindsight, this was where my faith in the “system” started to crack. Over the prior year, I had been reading a large volume the original published literature (not news - the medical journals) on the topic as I tried to make the best calls for our facility. I had seen nothing regarding vaccinating a just infected person but the university was quick to mandate this - even for a young healthy, just recovered patient. 25 years of clinical practice screamed that this was, at a minimum uncertain. We have never vaccinated against something that just occurred - it made no sense. But perhaps there was data that I had not seen? After all, they had multiple high ranking policy makers sitting on boards that, I assumed, had to have some level of insider information. I had been wrong before and could be wrong again. I would wait patiently but this event was the first large crack. The university pushed for ASAP vaccination - I was able to get her to delay the first vaccine dose until about 1 month post infection recovery. Within about 2 months of leaving university lockdown, she had both initial doses and thankfully tolerated them fine.
As the vaccine rollout continued during the first half of 2021, my spot in line came up. My initial vaccine was Moderna - did reasonably well with it I thought. I did get lightheaded driving home after the 20? min watch and wait period was over. I nearly had to pull over on the highway at one point due to an uneasy feeling and had a relatively bad headache intermittently for a few days. I was unable to exercise for about 1 week (part of my daily routine) due to worsening headaches with activity but I’d say I did ok - far worse than any flu annual vaccine (30+ yrs of those) but I was fine.
Second shot was due and I picked up my wife so I wasn’t driving solo home. At the time, I didn’t think too much of it, but in hindsight I guess even then I knew I felt bad after the first shot. I did seemingly fine in the period immediately following the shot but I ran a temp of around 100-102 for about 3 days post injection. Further, I had truly weird side effects - if I even grazed my hair, I got a bad headache. Several (5-10) times I sat down on stairs due to headaches in the 3 weekly post the second shot. I remember rolling down my car window a month or so later and had to roll it back up due to the wind causing this weird headache. I have a very low grade tinnitus and it worsened significantly in the weeks following shot #2. It would correspond to times when my headaches were more severe. I would roll over at night and hear rushing for 3-5 seconds loud enough to not sleep through. As I got farther out from the second shot, these episodes became less common. But on some level - they were clearly related to the vaccine.
After the first two vaccines, our family returned to a bit more normal schedule. We returned to church and began to travel a bit. Slowly returning towards the old normal. We had a ski trip scheduled for the winter of 2021. I knew it was relatively high risk but we had travelled very little and I was ready. About 1 month before the trip, Omicron landed. I waited for a few weeks to see about any data and as is expected with anything new, it was sparse. We waited as long as we could but about 2 weeks prior, I recommended myself and my wife get boosted. I had struggled with the Moderna vaccine and so I opted to “choose my own” via a large box store and boosted with Pfizer. It was about the only place I could find that let me pick my booster at the time. I knew the dosing for the two and I knew I had struggled and so I opted to get my healthcare - not at a healthcare facility but my first ever vaccine at big box store as my trust in the system moved a step down in the ladder relative to a trust in myself and my reading of the literature.
I’d say I did pretty well - a few headaches but much milder - but they were the same. I could gentle touch my hair and get a pretty significant pain - obvious and clearly different from anything I’ve experienced before or since. Tinnitus worsened again this time lasting longer - I’d say for a good 2-3 months with an episodic course.
The next large event came with the publication of this paper in January of 2022 - the CDC vaccine vs natural immunity. (Ref 3)
Crazy to think but this was the first time I had seen the government seem to admit on any level that prior infection did create very strong immunity and that, at that point it was at least as strong, if not stronger than vaccine immunity (not a lower risk path but if infected, you had good immunity). I want to be clear, I’m for vaccination and support boosters (especially in high risk cases), but up until this point the government refused to consider natural immunity and to talk about it made you a crazy person. I still remember reading this paper the day it was released and walking around clinic asking people if they had seen anything like this anywhere previously. This paper made me start to rethink many broad assumptions making up the largely unified voice mirroring the government stance and it gave me greater confidence that the decision that the university made earlier that year - essentially forcing a young healthy family member to be vaccinated as she recovered from the disease - had been done, not with data, but more as part of a marketing campaign for the university. I imagine it would have read: “We’re doing our part in leading the fight! Data be damned and we’ll use these kids to show just how serious we are!”
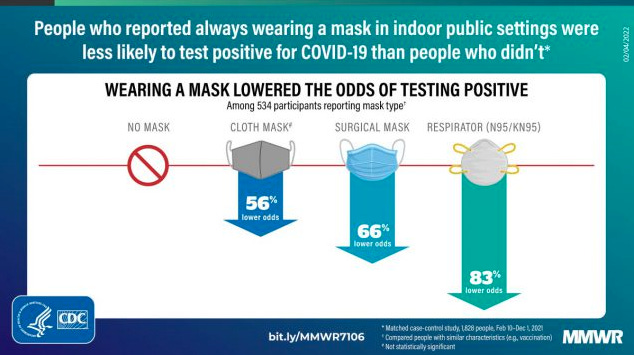
Over the course of 2021 and early 2022, the data continued to evolve - vaccines clearly wane, probably doesn’t offer much protection against infection, but continues to have severe disease risk reduction etc. etc. Yet the government and the CDC seemed to strengthen their stance - as if to make a point. It was somehow better to make absolute universal policy statements from children to elderly than to have discussions regarding risks and benefits. I remember the non-science marketing embarrassment shown below as a primary clear example of “science” gone wrong - a non-significant p value shows as a 56% reduction in risk. (Ref 4). (Yes there’s an asterisk with fine print but come on.)
We had come full circle. What Stephen Hahn (Radiation Oncologist from MD Anderson) had been held accountable for with a clear error or false statement in August of 2020 had become the stuff of marketing material for the CDC - only this time it was consistent with “approved” narrative.
Finally I’ll address two less clearly related items that have been part of my personal experience of the last few years. Firstly, I required blood pressure medication for the first time beginning in early 2022. It has been borderline for years but it ran higher then than before and it was higher then (6-12 months ago) than it is now. I honestly don’t know if this is related to the vaccines I received (in part) or not. It might be a side effect from the original trial data as shown as shown below (Ref 5 - really small numbers but that’s the issue with our paucity of randomized data). Secondly, in February of 2022, I had a ruptured appendix - no prior flares, out of blue my first ambulance ride in what went from a 2 mile run to a 911 call some 3 hours later. I’d say more likely unrelated but I’m not positive. In the months following the 2nd shot and the booster, I clearly had episodic multi-system inflammatory events - easiest to define by the hair / headache sensitivity. While I think a clear link is impossible to make, I think to state unequivocally that they are not related is as incorrect.
(I do want to be very careful here. I’m vaccinated and my family is all vaccinated. I believe strongly in vaccines. From my perspective, they were the most important development that changed the trajectory of this disease and it was a travesty that they were politicized on any level. But we should have far better data. We should have run far more randomized trials. We should have looked closely for toxicities in prospective trials - especially outside of the highest group populations so that there would be less questioning.)
Simply stated for two years I was medical director of a large healthcare facility through the pandemic. I lost countless hours of sleep worrying about the cancer patients and the facility as we tried to navigate an extremely difficult time in our history. I know science and I read hundreds of original reference articles on COVID. I watched as historically trustworthy departments, institutions, and journals published lower and lower quality data in what appeared, at least to me, an attempt to meet a narrative.
To date, the US has generated near zero randomized data on most everything COVID related. From March of 2020 until today - nearly 3 years into a worldwide pandemic, we have politicized the answer without performing due diligence in the science. I’m certain we ran far too few trials and achieved randomized answers on far too few topics and these inactions will forever stain this period of time. From my perspective, we have all seen money and power win over science even within the “science” community. There are now pockets of discussion regarding these important topics but in my opinion, there has been far too little and it was “allowed” far too late.
To be fair, I stayed quite. I considered going to the news regarding the non-call CT reading of the COVID diagnosis. It was wrong and it put two patient populations at risk. That said, I also knew the likely outcome. I’ve been around the block and been in many an administrative meetings. At best the “change” would have been a middle to upper tier radiology physician being let go or some internal shuffling of radiology staff. The administration and hospital would have simply rolled forward with a fresh marketing campaign on their great diligence in handling this new disease. I might have created a day or two of chaos, but little real impact and therefore, I opted against that uphill path.
Moving forward, I’ll continue to be independent. I’ll continue to read current literature with a science based approach and I will purposefully work to follow my reading of the literature and trust what I see in my clinic and I’ll be one step less inclined to follow the national narrative. Radiation Oncology has many current narratives - many of which I believe have been very detrimental to our field over the last 20 years. At times, I started to believe or consider some of them, but the last 2 years have made me refocus. It is far too easy in today’s world to follow group-think. Nearly 4 years ago, I opted to explore proton therapy as a way to help determine first hand if this a useful tool for cancer patients. There is no doubt that these two experiences (the jump to a proton facility and COVID) have shaped how I will evaluate medical decisions in the future. That will be a main focus of this Substack.
A final quick story. Just last week I was trying to look up a reference document for a patient and the top three references were from the CDC. I skimmed past those moving onto a variety of other references to try and determine the correct answer. It was subconscious at first, but then, it wasn’t. At the end of the day, I think the damage done to our institutions and to our healthcare system was massive when some level of humility and some acknowledgement of our uncertainty would have served us far better.
Why here on Substack:
I’m starting here on Substack as I think it affords one more layer of separation from my medical practice. Rather than posting on my old blog sat on the same domain as my practice information site, I thought it would be best to bring these posts here.
REFERENCES:
The Predictive theory of COVID-19
Modeling and error journey during COVID by Alex Washburne
Washington University 2020 COVID model links:
News story: https://www.washington.edu/news/2020/04/10/covid-19-peak-active-cases/
Actual current version of site: https://covid19.healthdata.org/united-states-of-america?view=cumulative-deaths&tab=trend
Natural Immunity CDC paper: https://www.cdc.gov/mmwr/volumes/71/wr/mm7104e1.htm#F1_down
Mask graphic:
Moderna Original Trial supplemental data:
https://www.nejm.org/doi/suppl/10.1056/NEJMoa2035389/suppl_file/nejmoa2035389_appendix.pdf